Introduction
Congenitally missing permanent teeth are common in patients with clefts. This retrospective study was conducted to evaluate the craniofacial characteristics in patients with unilateral complete cleft lip and palate with congenitally missing permanent teeth.
Methods
A series of 73 consecutive patients with nonsyndromic unilateral complete cleft lip and palate were enrolled. Evaluation of congenitally missing permanent teeth was based on the panoramic films taken from 7 to 11 years of age. The cephalometric films taken around 9 years of age were used to compare the craniofacial morphology in patients with no congenitally missing permanent teeth (n = 20) and 1 (n = 25), 2 (n = 18), and 3 (n = 10) congenitally missing permanent teeth. The Spearman correlation coefficient was used to assess the association of increased numbers of congenitally missing permanent teeth with each cephalometric parameter.
Results
Anterior facial height, distance from the maxillary incisor and first molar to the palatal plane, and overjet decreased as the number of congenitally missing permanent teeth increased in patients with unilateral cleft lip and palate.
Conclusions
Unilateral cleft lip and palate patients with congenitally missing permanent teeth have a unique craniofacial morphology with a reduced vertical dimension.
Maxillary growth in patients with cleft lip and palate is often restricted. The causes of growth inhibition come from 2 main factors: the iatrogenic factor resulting from surgical repair of the cleft lip and palate, and the intrinsic developmental deficiency in cleft patients. Numerous studies have been conducted to search for the parameters of the intrinsic factors of maxillary growth in cleft patients. These parameters include cleft size, premaxillary size, palatal surface area, and number of congenitally missing permanent teeth. Median facial dysplasia is a subgroup of cleft lip and palate, which is characterized by midline facial deficiency, short columella, hypoplastic maxilla, and congenitally missing maxillary permanent incisors. Patients with an alveolar cleft exhibit a deficiency in mesenchymal mass, which can result in the absence of teeth.
There are 2 reasons that cleft patients are susceptible to congenitally missing permanent teeth. The first reason is the adjacency of the cleft and the dental lamina formation. The orofacial cleft is formed by failure of the maxillary process to fuse with the medial nasal process. The oral epithelium on the primary processes forms the dental laminae, which develop into tooth germs. The second reason is the timing of cleft development and tooth germ formation during the fifth to seventh weeks of embryogenesis.
In previous studies, missing teeth have been shown to have a relationship with craniofacial morphology in noncleft patients. A tendency to develop a Class III skeletal relationship was noted in patients with congenitally missing permanent teeth. Several studies showed an association of congenitally missing permanent teeth with craniofacial morphology, including decreased dentoalveolar support (decreased SNA, SNB, ANB, and lower anterior facial height) and functional compensation (decreased mandibular plane angle), rather than a different growth pattern. The variables—eg, cranial base length and angle, maxillary length, mandibular length, and upper facial height in patients with congenitally missing permanent teeth—were not different compared with subjects without congenitally missing permanent teeth. The functional compensation for counterclockwise rotation of the mandible results from reduced dentoalveolar support and a skeletal Class III tendency in subjects with more congenitally missing teeth (>6-10). However, the association of missing teeth and growth impairment has not been adequately documented in studies of cleft patients. Thus, a study to explore the relationship between craniofacial morphology and congenitally missing permanent teeth in patients with cleft lip and palate is necessary.
Studies in the last decade have shown that genetic factors play important roles in congenitally missing permanent teeth. Some genes might contribute to both orofacial clefting and congenitally missing permanent teeth. Animal models of mice show that the lack of the MSX1 gene (muscle segment homeobox) function induces cleft palate, deficient alveolar bones, and failure of tooth development. In addition to MSX1 , mutation in PAX9 (paired box gene 9) has been associated with nonsyndromic tooth agenesis in humans. PAX9 and MSX1 double homozygous mutants exhibit an incomplete penetrant cleft lip phenotype. Moreover, the mandibular incisors are consistently missing in double heterozygous mutants of PAX9 and MSX1 . The IRF6 (interferon regulatory factor-6) gene is associated with the Van der Woude syndrome, lip pit, and tooth agenesis. The PVRL1 (poliovirus receptor related-1) gene is responsible for the cleft lip and palate-ectodermal dysplasia syndrome.
Based on the embryologic and genetic viewpoint in patients with orofacial clefting, we speculated whether the number of congenitally missing permanent teeth would be an indicator of an intrinsic deficiency of maxillary growth in patients with clefts. Knowing the relationship of congenitally missing permanent teeth to craniofacial morphology in cleft patients might help to predict their future growth and anticipate their treatment needs.
Material and methods
Patient records were retrieved from the database of Chang Gung Craniofacial Center, Taipei, Taiwan. The inclusion criteria were as follows: Taiwanese patients with unilateral complete cleft lip, alveolus, and palate; consecutive patients in Chang Gung Memorial Hospital born between 1994 and 1995; and patients with complete records from about 7, 9, and 11 years, including panoramic and occlusal radiographs, intraoral photographs, and clinical dental charts. These patients received the standard cleft treatment protocol in the craniofacial center.
The following exclusion criteria were used: patients who had orthodontic or orthopedic treatment, such as facemask and palatal expansion (except prealveolar bone grafting orthodontic treatment, which is alignment of the maxillary teeth only); or patients who had extractions of permanent teeth.
There were 273 consecutive patients with complete unilateral cleft lip and palate born between 1994 and 1995. Among them, 107 patients had no 7-year records, and 71 patients had no 9-year records. Four patients did not receive lip repair at the Chang Gung Craniofacial Center, 2 patients had congenital heart disease, 2 patients had median facial dysplasia, and 14 patients had incomplete cleft lip or alveolus. All of these patients were excluded. Therefore, only 73 patients were included in this study.
The 73 patients were divided into 4 groups according to the number of congenitally missing permanent teeth in the maxillary dentition: no congenitally missing permanent teeth (group 0, n = 20), 1 congenitally missing permanent tooth (group 1, n = 25), 2 congenitally missing permanent teeth (group 2, n = 18), and 3 congenitally missing permanent teeth (group 3, n = 10). The sex and age distributions in each group are listed in Table I . The maxillary lateral incisor was diagnosed as present on either the mesial or the distal side of the cleft, regardless of tooth morphology. When more than 1 lateral incisor was observed, the distal one (if the tooth sizes were similar) or the smaller one was identified as the supernumerary tooth. All patients were treated according to the standard protocol for cleft treatment between 1992 and 1996. They wore a feeding plate for 3 months before lip repair and received primary cheiloplasty and rhinoplasty at the age of 3 to 6 months. Two-flap palatoplasty was performed at about 9 to 12 months of age. The patients were followed regularly after the primary plate repair. If persistent velopharyngeal insufficiency with hypernasal speech was diagnosed, secondary palatal repair was conducted to correct it around the age of 4 to 5 years. The techniques used for secondary palatal repair were individualized. Alveolar bone grafting was done at 9 years of age, and the bone graft was harvested from the iliac crest. The criteria to receive presurgical orthodontic treatment before alveolar bone grafting were based on the local condition of surgical accessibility. The purposes of orthodontic treatment were to level and align the gingivae of the 2 segments in the alveolar process and to correct the malpositioned maxillary incisors. The presurgical orthodontic treatment in the selected patients facilitated the surgical access and primary closure in alveolar bone grafting.
| Group 0 (n = 20) | Group 1 (n = 25) | Group 2 (n = 18) | Group 3 (n = 10) | P value | |
|---|---|---|---|---|---|
| Sex, n (%) | |||||
| Male | 13 (65) | 15 (60) | 14 (78) | 6 (60) | 0.603 |
| Female | 7 (35) | 10 (40) | 4 (22) | 4 (40) | |
| Mean age | 9 y | 9 y 1 mo | 9 y | 9 y | |
| Range | 8 y 5 mo-9 y 8 mo | 8 y 8 mo-9 y 10 mo | 8 y 1 mo-9 y 8 mo | 8 y 6 mo-9 y 4 mo | 0.640 |
| Missing teeth (FDI tooth numbers) | – | 12 or 22 or 21 | 12, 22 or 12, 25 or 15, 22 or 22, 25 or 13, 25 or 24, 25 | 12, 22, 25 or 12, 22, 15 |
Other parameters that were considered as possible causes of growth inhibition were also investigated to determine their contribution to the craniofacial growth and to clarify their association with congenitally missing permanent teeth. The parameters included the alveolar cleft width and whether the patients had undergone secondary palatoplasty.
The patients’ medical chart, intraoral photographs, and x-ray films were reviewed and analyzed by the same investigator (T.-T.W.) and further validated by the senior investigator (E.W.-C.K.).
The clinical records from the medical chart included the following: surgical technique, names of surgeons who performed the cheiloplasty and the palatoplasty, initial alveolar cleft width, and history of permanent tooth extractions.
The width of alveolar cleft was measured directly using a sliding caliper in the first visit, before the patient began wearing the feeding plate.
The diagnosis of congenitally missing permanent teeth was based on the collaboration judgment from the panoramic radiographs, occlusal radiographs, intraoral photographs, and clinical dental charts. The anterior permanent teeth (canine and incisor) were evaluated based on the records from 7 to 9 years of age to reduce the misinterpretation of counting the extracted peg lateral incisors or supernumerary teeth as missing because some peg laterals might have been extracted at an early age. The panoramic films from 11-year-old patients were used to evaluate the missing posterior teeth (premolars and molars) because some second premolars develop late after ages 6 and 7 years. Furthermore, patients with cleft lip and palate often have delayed tooth development compared with the noncleft population. Hence, the observation of premolars was further confirmed by the panoramic films taken about 11 years of age. This diagnostic procedure can prevent misinterpretation of congenitally missing permanent teeth because of early extractions and late mineralization of the permanent teeth.
The lateral and posteroanterior cephalometric radiographs taken of 9-year-old patients were traced and analyzed. The x-ray films were taken either before or shortly after secondary alveolar bone grafting, which was performed about 9 years of age. The reason for selecting the 9-year records to document the facial dimension was that maxillary growth was not deleteriously affected by the secondary alveolar bone grafting before or during the first postoperative year after the grafting. The data were more complete for the 9-year records of the patients in our database.
All cephalometric radiographs were taken with the patients in natural head position and the teeth in centric occlusion. The radiographs were taken with a Panelipse dental x-ray machine (General Electric, Milwaukee, Wis), set at 75 kV, 10 mA, and 2 seconds of exposure time. The magnification ratio at the midsagittal plane was 10.74% in the cephalometric film.
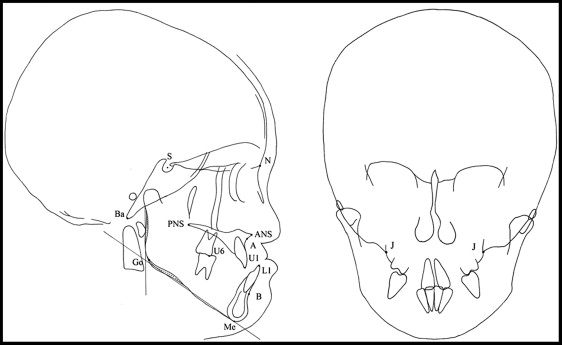
The landmarks and reference planes in the cephalometric radiographs are listed in Figure 1 . The measurements of linear distances in the cephalometric analysis were calibrated to actual distances for the statistical tests.
For the error study, 10 randomly selected lateral and posteroanterior cephalometric films were traced and measured twice in a 1-month interval. Dahlberg’s formula, √(∑D 2 /2N), was used to assess random errors of the linear and angular measurements. The random errors of these measurements ranged from 0.29 to 0.72 mm and 0.55° to 1.43°, respectively. Two paired t tests with a 95% confidence interval showed no systematic measurement errors ( P >0.05).
Statistical analysis
The Spearman rank correlation coefficient was used to calculate the association of the increase in the numbers of congenitally missing permanent teeth and the width of the alveolar cleft on each cephalometric parameter. For comparisons of patients with and without the secondary palatoplasty, Mann-Whitney U tests were used to compare the differences. Any statistically significant parameter was subsequently incorporated into the multiple linear regressions.
A 2-sided P value below 0.05 was considered statistically significant. Data were analyzed using the Statistical Package for the Social Science (version 17.0 for Windows; SPSS, Chicago, Ill).
This study was approved by the institutional review board and medical ethics committee at Chang Gung Memorial Hospital. Helsinki Declaration guidelines were followed.
Results
The age to obtain the cephalometric analysis of these patients ranged from 8 years 1 month to 9 years 10 months. The mean age was 9 years. The surgeries of cheiloplasty and palatoplasty were done by the same craniofacial team. The distributions of sexes, ages, and surgeons of cheiloplasty and palatoplasty were not significantly different among the 4 groups ( Table I ).
The cephalometric measurements of skeletal and dental variables in the 4 patient groups and the associations between hypodontia and craniofacial morphology are listed in Table II .
| Group 0 (n = 20) | Group 1 (n = 25) | Group 2 (n = 18) | Group 3 (n = 10) | P value | Spearman correlation coefficient | |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| SN (mm) | 65.1 ± 3.4 | 66.3 ± 3.1 | 64.8 ± 3.4 | 64.1 ± 3.7 | 0.491 | −0.082 |
| SBa (mm) | 44.7 ± 2.3 | 45.1 ± 2.4 | 44.8 ± 2.6 | 44.3 ± 1.9 | 0.703 | −0.045 |
| NSBa (°) | 129.9 ± 3.8 | 129.9 ± 5.2 | 130.6 ± 4.5 | 129.4 ± 4.7 | 0.885 | 0.017 |
| SNA (°) | 78.7 ± 3.8 | 77.1 ± 3.9 | 77.1 ± 3.2 | 80.1 ± 4.7 | 0.707 | −0.045 |
| SNB (°) | 77.9 ± 3.3 | 77.1 ± 3.9 | 77.0 ± 3.6 | 79.8 ± 5.0 | 0.706 | 0.045 |
| ANB (°) | 0.8 ± 3.1 | −0.1 ± 3.5 | 0.1 ± 3.1 | 0.2 ± 2.8 | 0.664 | −0.052 |
| N-ANS (mm) | 50 ± 3.3 | 50.4 ± 3.0 | 49.5 ± 2.4 | 48.1 ± 2.6 | 0.298 | −0.124 |
| ANS-Me (mm) | 61.9 ± 3.3 | 63.0 ± 4.3 | 60.6 ± 2.9 | 58.7 ± 5.0 | 0.044 ∗ | −0.237 |
| N-Me (mm) | 111.1 ± 5.1 | 112.3 ± 4.1 | 109.8 ± 4.4 | 106.2 ± 7.0 | 0.077 | −0.208 |
| S-PNS (mm) | 43.4 ± 2.5 | 43.4 ± 2.9 | 42.5 ± 2.5 | 42.4 ± 3.4 | 0.146 | −0.172 |
| S-Go (mm) | 70.4 ± 3.9 | 70 ± 4.1 | 67.7 ± 3.8 | 68.9 ± 4.6 | 0.071 | −0.213 |
| SN-MP (°) | 34.7 ± 5.5 | 35.9 ± 4.5 | 36.0 ± 4.4 | 31.4 ± 5.9 | 0.557 | −0.070 |
| SN-PP (°) | 10.1 ± 3.7 | 10.0 ± 3.6 | 10.5 ± 2.6 | 9.7 ± 2.6 | 0.896 | 0.016 |
| PNS-ANS (mm) | 46.1 ± 2.4 | 45.9 ± 3.3 | 44.8 ± 1.9 | 45.4 ± 3.1 | 0.310 | −0.121 |
| PNS-A (mm) | 43.1 ± 2.3 | 42.8 ± 3.2 | 42.1 ± 1.8 | 42.9 ± 2.9 | 0.386 | −0.103 |
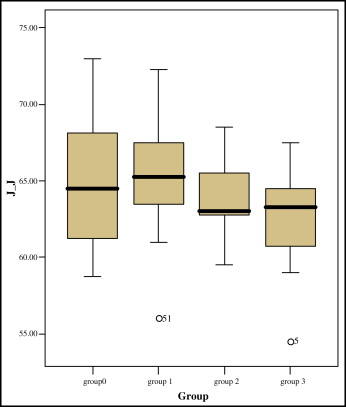
| J-J′ (mm) | 64.6 ± 4.2 | 64.9 ± 3.7 | 63.8 ± 2.5 | 62.4 ± 3.6 | 0.190 | −0.156 |
| U1-SN (°) | 100.8 ± 6.4 | 98.3 ± 7.1 | 96.7 ± 9.1 | 97 ± 11.1 | 0.188 | −0.156 |
| L1-MP (°) | 92.1 ± 6.9 | 90.1 ± 7.9 | 92.5 ± 8.7 | 91.8 ± 7.8 | 0.895 | −0.016 |
| U1-PP (mm) | 25.4 ± 2.6 | 25.8 ± 2.1 | 24.5 ± 2.0 | 22.7 ± 2.7 | 0.004 † | −0.333 |
| U6-PP (mm) | 19.7 ± 2.0 | 20.2 ± 2.0 | 19.1 ± 1.1 | 18.4 ± 2.6 | 0.029 ∗ | −0.259 |
| Overbite (mm) | 3.2 ± 2.6 | 3.2 ± 3.2 | 3.0 ± 2.2 | 3.2 ± 2.3 | 0.900 | −0.015 |
| Overjet (mm) | −1.1 ± 2.3 | −0.9 ± 2.8 | −2.7 ± 3.1 | −2.7 ± 2.8 | 0.047 ∗ | −0.233 |
The lengths of the anterior cranial base, posterior cranial base, and cranial base angle were not associated significantly with the numbers of congenitally missing permanent teeth ( P >0.05).
Upper anterior facial height was not associated statistically with the number of congenitally missing permanent teeth ( P = 0.298). However, the scatter plot highlighted a tendency of decreasing upper anterior facial height as the number of congenitally missing permanent teeth increased ( Fig 2 , A ).

Lower anterior facial height was statistically significant in its association with the number of missing teeth ( P = 0.044, r = −0.237; Fig 2 , B ).
Anterior facial height was not associated statistically with the number of congenitally missing permanent teeth ( P = 0.721). However, the scatter plot showed a tendency of decreasing anterior facial height as the number of missing teeth increased ( Fig 2 , C ).
For the sagittal dimensions, maxillary protrusion, mandibular protrusion, intermaxillary relation, maxillary length, and maxillary alveolar length were not associated with the number of congenitally missing permanent teeth ( P >0.05).
For the transverse dimension, alveolar maxillary width was not associated significantly with the number of congenitally missing permanent teeth ( P = 0.190). However, the scatter plot highlighted a tendency of decreasing alveolar maxillary width as the number of missing teeth increased ( Fig 3 ).
The distance from the maxillary incisor to the palatal plane was statistically significantly associated with the severity of congenitally missing permanent teeth ( P = 0.004, r = −0.333; Fig 4 , A ).

The distance from the maxillary first molar to the palatal plane was statistically significantly associated with the number of congenitally missing permanent teeth ( P = 0.029, r = −0.259; Fig 4 , B ).
Overbite was not associated with the number of congenitally missing permanent teeth ( P = 0.900). However, overjet was significantly associated with the number of congenitally missing permanent teeth ( P = 0.047, r = −0.233; Fig 4 , C ). As the number of congenitally missing permanent teeth increased, overjet was reduced.
Mann-Whitney U tests were used to compare upper anterior facial height, anterior facial height, lower anterior facial height, maxillary incisor to palatal plane, maxillary first molar to palatal plane, overjet, and alveolar maxillary width between groups 0 and 1. No significant differences were identified ( P >0.05).
Other possible confounding factors, including alveolar width and secondary palatoplasty, are described below.
The correlation between the width of the alveolar cleft and craniofacial morphology was assessed with the Spearman rank correlation coefficient test, which showed that no cephalometric measurements were associated with the width of the alveolar cleft before alveolar molding ( P >0.05) ( Table III ).


