Correction of a severe protrusive soft tissue profile without orthognathic surgery can be challenging. This case report describes the treatment of a young woman with a severe bimaxillary protrusion. Orthodontic treatment included extraction of her 4 first premolars and total arch distalization of both arches using a palatal plate appliance. The total treatment time was 24 months. Her occlusion and facial appearance were significantly improved.
Highlights
- •
A young woman with bimaxillary protrusion sought treatment.
- •
Profile improvement after premolar extraction treatment was not satisfactory.
- •
Additional total distalization by palatal plate corrected the severe protrusion.
- •
This treatment modality might be a feasible option for bimaxillary protrusion.
Bimaxillary dentoalveolar protrusion is a common dentofacial deformity that results in functional and esthetic problems that traditionally were treated with premolar extractions. Patients with severe bimaxillary dentoalveolar protrusion are often treated with a combination of orthodontics and orthognathic surgery to improve the facial profile.
In severe cases of protrusion, the typical orthodontic therapy that includes extraction of the 4 first premolars and retraction of anterior teeth may not be sufficient to improve the facial profile. Schacter and Schacter reported that extracting both premolars in the same quadrant can generate enough space to alleviate severe crowding and allow incisor retraction to treat the bimaxillary protrusion and create contact between the canine and the first molar. However, this approach might lead to loss of the premolars’ function and cause periodontal problems and disturbances in the occlusion. Therefore, total arch distalization might be required to supplement the extraction treatment if patients decline surgical options to improve their profiles.
Currently, it is being suggested that temporary skeletal anchorage devices can be used to support molar distalization devices. However, placing temporary skeletal anchorage devices in the buccal plate of bone poses a higher risk of contacting the roots of adjacent teeth and a limited range of action because of the interradicular space. Therefore, a modified palatal anchorage plate (MPAP) may overcome this drawback and effectively distalize the whole dental arch.
This case report presents a young woman with a severe bimaxillary protrusion treated with 4 first premolar extractions and total arch distalization with a palatal anchorage plate.
Diagnosis
A young woman, aged 20 years 4 months, came to the orthodontic department of Seoul St. Mary’s Hospital, Catholic University of Korea, in Seoul with the chief complaint of lip protrusion. Her lips were incompetent because of the severe proclination of her maxillary incisors at rest. When smiling, the left side of her upper lip lifted more than the right. No significant skeletal asymmetry or temporomandibular joint disease was found. She was healthy, with no specific medical problems.
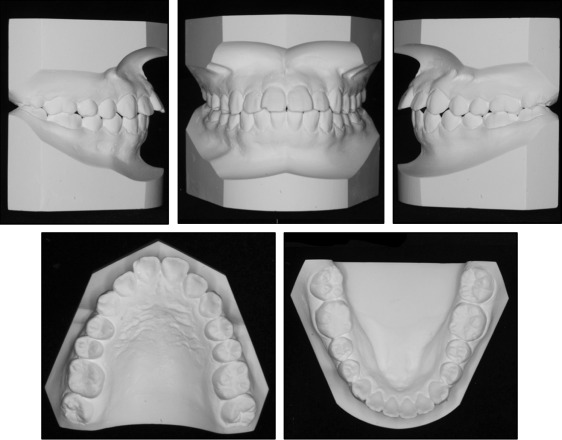
She had an overjet of 6.5 mm, a 10% overbite, and mild crowding in both arches. She had Class I molar relationships and dental caries on her mandibular second molars ( Figs 1 and 2 ). The panoramic radiograph showed a missing mandibular left third molar, and her other third molars were in the developmental stage ( Fig 3 , A ).

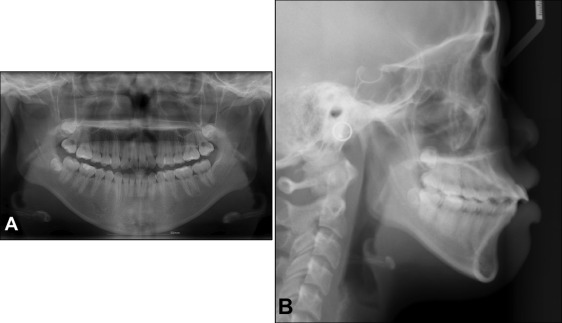
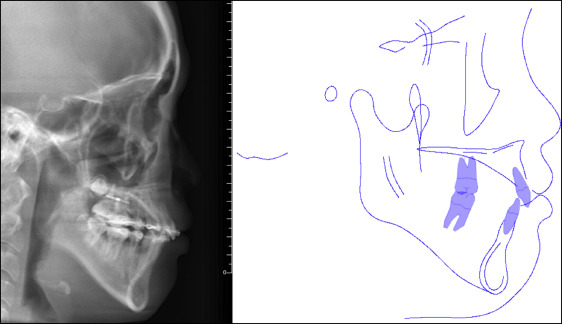
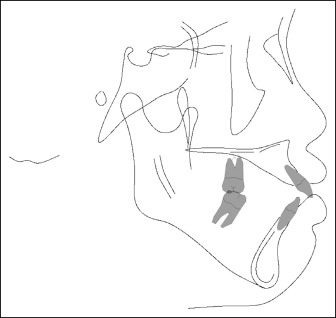
The lateral cephalometric analysis indicated a skeletal Class I pattern (ANB, 3.5°; Wits appraisal, −1.0 mm) with a hyperdivergent growth pattern (FMA, 33.0°). The maxillary and mandibular incisors were proclined (U1-FH, 135.0°; IMPA, 94.5°; U1/L1, 97.5°). The upper and lower lips were protrusive (upper lip to E-line, 2.5 mm; lower lip to E-line, 5.0 mm) with an acute nasolabial angle (79.0°). She had a short upper lip (subnasale-stomion, 17.0 mm) with an increased ratio of lower lip and chin to upper lip (stomion-soft tissue menton/subnasale-stomion, 3.0) ( Figs 3 , B , and 4 ; Table ).
| Measurement | Norm ± SD | Pretreatment | Progress (after maximum retraction) | Posttreatment |
|---|---|---|---|---|
| SNA (°) | 82.0 ± 2.0 | 83.5 | 83.5 | 83.5 |
| SNB (°) | 80.0 ± 2.0 | 80.0 | 79.5 | 78.0 |
| ANB (°) | 3.5 ± 1.9 | 3.5 | 4.0 | 5.5 |
| Wits (mm) | −2.5 ± 1.8 | −1.0 | −0.8 | −0.5 |
| Harvold (mm) | 26 ± 4.0 | 34.0 | 33.9 | 33.3 |
| FMA (°) | 22 ± 3.0 | 33.0 | 34.5 | 36.0 |
| U1-FH (°) | 114 ± 6.5 | 135.0 | 110.0 | 100.0 |
| U1-APog (mm) | 7.8 ± 2.2 | 14.0 | 5.5 | 2.5 |
| IMPA (°) | 91.6 ± 2.0 | 94.5 | 81.0 | 75.0 |
| L1-NB (mm) | 3 ± 2.0 | 10.0 | 6.5 | 4.0 |
| U1/L1 (°) | 124 ± 8.3 | 97.5 | 130.0 | 148.0 |
| E-line–upper lip (mm) | −1.2 ± 2.2 | 2.5 | 1.5 | 0.5 |
| E-line–lower lip (mm) | 0.14 ± 2.8 | 5.0 | 2.0 | 1.0 |
| Nasolabial angle (°) | 84.9 ± 5.0 | 79.0 | 89.0 | 92.0 |
| TVL-UL (mm) | 3.7 ± 1.2 | 9.5 | 6.7 | 6.5 |
| TVL-LL (mm) | 1.9 ± 1.4 | 10.0 | 4.5 | 2.5 |
| TVL-Pog′ (mm) | −2.6 ± 1.9 | 2.5 | 0.0 | −2.0 |
| Sn-Stm (mm) | 22.6 ± 2.1 | 17.0 | 17.0 | 20.0 |
| Stm-Me (mm) | 48.8 ± 3.3 | 43.5 | 43.5 | 43.0 |
| Stm-Me/Sn-St (ratio) | 2.0 ± 0.2 | 3.0 | 3.0 | 2.5 |
| PTV-UL (mm) | 68.0 | 65.0 | 63.5 | |
| PTV-LL (mm) | 68.0 | 64.5 | 59.5 | |
| PTV-Pog′ (mm) | 64.5 | 59.5 | 54.5 |
Treatment alternatives
The first treatment option was to perform an anterior segmental osteotomy combined with first premolar extractions because of her thin anterior alveolus. The second treatment option was to fully retract her anterior teeth after extraction of her first premolars. However, if the improvement in her profile was not satisfactory after closure of the extraction space, a further treatment option was to distalize the entire maxillary dentition using a palatal plate appliance. The mandibular dentition would be distalized along with the maxillary dentition using Class III elastics.
The patient refused the surgical treatment option. Therefore, the second and the additional treatment options were used to improve her profile.
Treatment progress
Before orthodontic treatment, the patient was referred to a general dentist for treatment of the dental caries and extraction of all first premolars. She was also sent to an oral surgeon to evaluate the extraction of her third molars, but she declined the extractions. Preadjusted appliances with 0.022-in slots were bonded on both arches for leveling and alignment. Her maxillary arch was leveled with archwires, starting with 0.016-in nickel-titanium and working up to 0.019 × 0.025-in stainless steel wires. Two miniscrews were placed between the maxillary first and second molars for maximum anchorage. The maxillary and mandibular anterior teeth were retracted en masse using 0.019 × 0.025-in stainless steel wires with hooks between the lateral incisors and the canines for 7 months. Unfortunately, even after retraction of the maxillary anterior segment with maximum anchorage, the patient still had protrusive lips ( Fig 5 ).