8 Contemporary removable appliances
Tooth movement with removable appliances
Removable appliances are also useful in maintaining tooth positions during retention.
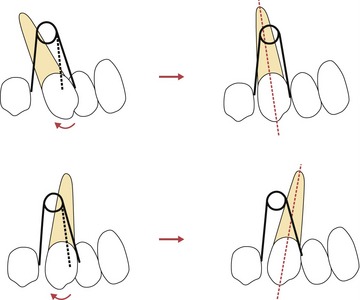
Tipping
Unlike fixed appliances, which can control the movement of a tooth in three dimensions, the force applied by a removable appliance is mediated by a spring, elastic or piece of acrylic, which can only make point contact with the tooth. As no reactionary force or couple is created, in these situations removable appliances are only capable of simple tooth tipping and apical or bodily movement is not possible. Tipping can be carried out in mesial, distal, buccal or lingual directions, with the rotation occurring about a fulcrum located close to the middle of the tooth root. For the retraction of teeth already mesially inclined, tipping can be an effective tooth movement; but it is inappropriate for teeth that are upright or distally inclined (Fig. 8.1).
Extrusion
A whip-spring or elastic from a removable appliance can be used to extrude teeth by engaging a fixed attachment on a tooth to generate a vertical component of force. This can be useful for extrusion of an impacted central incisor in the mixed dentition (see Fig. 10.22).

Components of removable appliances
Removable appliances are composed of retentive and active components connected together by a baseplate. When designing a removable appliance, consideration also needs to be given towards anchorage, ensuring that the desired teeth will move under the active force applied by the appliance (Box 8.1).
Retentive components
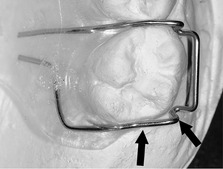
Adams clasp
Adams clasps are constructed in 0.7-mm stainless steel wire and most commonly used on the first molars (Fig. 8.3), although they can be used on premolars and anterior teeth. The arrowheads of the clasp engage undercuts at the mesial and distal corners of the buccal tooth surface and can easily be adjusted at the chairside to increase retention. The bridge of an Adams clasp can also be used by the patient to remove the appliance from the mouth, whilst the orthodontist can use it to attach auxiliary springs or tubes for headgear.
Southend clasp
The Southend clasp is also constructed in 0.7-mm stainless steel wire, but is used for retention on the incisor teeth (Fig. 8.4). This clasp is activated by bending the U-loop towards the baseplate, which carries the clasp back into the labial undercut of the tooth.

Ball-ended clasp
Ball-ended clasps engage into interproximal undercuts between the teeth (Fig. 8.5) and are activated by bending the ball towards the contact point.

Plint clasp
Plint clasps are useful when using a removable appliance in combination with a fixed appliance (Fig. 8.6). These clasps are constructed in 0.7-mm stainless steel and engage the undercuts on a maxillary molar band.

Labial bow
A labial bow is constructed from 0.7-mm stainless steel wire and can provide retention from the labial surface of the incisor teeth, which can be increased by contouring the wire around these teeth in a fitted labial bow or by placing an acrylic facing on the wire of the bow (Fig. 8.7). The labial bow is afforded flexibility by incorporating U-loops at each end, which allow activation by compression.

Active components
Springs
Mechanical principles should be considered when applying a force to any tooth with a spring:

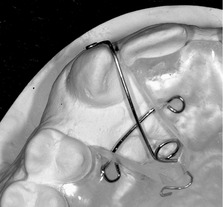
Palatal finger springs
Palatal finger springs are constructed in 0.5- or 0.6-mm stainless steel wire and used to move teeth mesially or distally along the dental arch (Fig. 8.8). The incorporation of a helix increases the length of the wire and allows the delivery of lighter forces whilst a guard wire will protect the spring from distortion. By convention, the helix is placed such that activation of the spring is achieved as it is tightened and it unwinds as tooth movement occurs; the spring should be positioned at right angles to the planned tooth movement.
Buccal canine retractor
Buccal canine retractors are constructed in 0.7-mm stainless steel, reduced to 0.5-mm if sheathed (Fig. 8.9). These springs can be used to retract buccally placed maxillary canines; however, when activated it is mechanically difficult to apply force directly to the mesial surface of the tooth.

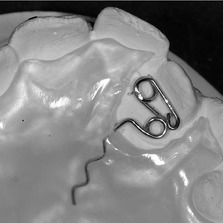
Z-spring
The Z-spring is constructed in 0.5-mm stainless steel wire and generally used to move one or two teeth labially (Fig. 8.10). Activation is achieved by pulling the spring away from the baseplate at an angle of approximately 45°, which will tend to displace the appliance away from the palate; good anterior retention is therefore important.
T-spring
T-springs are constructed in 0.5-mm stainless steel wire and used to move individual teeth either labially or buccally (Fig. 8.11). Activation is again produced by pulling the spring away from the baseplate and therefore retention also needs to be good.
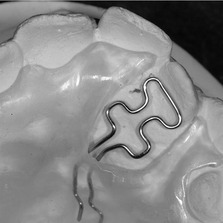
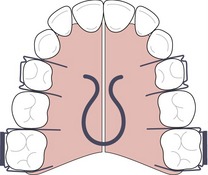
Coffin spring
A coffin spring provides a useful alternative to a screw for expansion (Fig. 8.12). This heavy spring is constructed in 1.25-mm wire and activated by pulling the two halves of the appliance apart manually or flattening the spring with pliers. Coffin springs deliver high forces that will tend to displace the appliance and good retention is important.
Active labial bows
An active labial bow can be used to reduce an increased overjet by tipping the teeth palatally if the upper labial segment is proclined and spaced. However, a normal labial bow will only allow a small range of activation and this can be improved either by increasing the amount of wire in the bow, as in a Mills bow, or by constructing it in a lighter wire, such as a Roberts retractor (Fig. 8.13). The Roberts retractor is constructed in 0.5-mm stainless steel with buccal arms sheathed in stainless steel tubing. Activation occurs by bending the vertical arms of the bow towards the palate and trimming the acrylic behind the upper incisors to allow palatal movement.

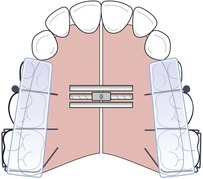
Screws
Screws can be embedded into the baseplate of an appliance and activated by the patient progressively turning a key (Fig. 8.14). Screws can be effective for expansion to correct a posterior dental crossbite, or for distal movement of the buccal segments, often supported by headgear. Each quarter turn of the screw activates it by approximately 0.2-mm and, therefore, should be done by the patient once or twice a week.
Elastics
Elastomeric forces can also be applied from a removable appliance and these can be useful in providing light force, which can be reactivated regularly by the patient. Intra-arch elastics can be used to retract the upper incisors as well as applying an intrusive force in patients with reduced periodontal support (see Fig. 8.2). Inter-arch application of elastics from removable appliances requires good retention to avoid displacement and is generally avoided.
Removable appliance design and use
Comprehensive orthodontic treatment is no longer undertaken with removable appliances alone because the results are invariably inferior to those produced by fixed appliances. However, removable appliances are relatively simple to use (Table 8.1), generally well tolerated by patients and can be used very effectively to correct minor occlusal problems (such as crossbites) in the mixed dentition or provide a valuable adjunct to fixed appliance therapy.
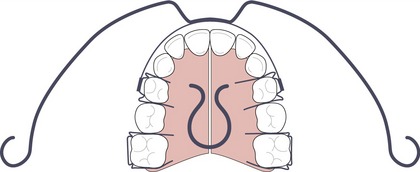
Expansion
Removable appliances can provide an effective method for expanding the maxillary dental arch, particularly in the mixed dentition (Fig. 8.14):
Correction of anterior crossbite
Removable appliances are also effective at correcting an anterior crossbite (Fig. 8.15). Palatal Z- or T-springs can be used to correct one or two teeth in anterior crossbite, usually in conjunction with posterior acrylic capping to open the bite and allow movement of the teeth out of crossbite. Occasionally some anterior retention in the form of a Southend clasp may also be required (Fig. 8.16).


Bite plane
In a growing patient, the incorporation of a flat anterior bite plane in a removable appliance allows eruption of the posterior teeth and reduction of a deep overbite (see Fig. 11.15). It can also facilitate earlier placement of a lower fixed appliance without impinging on the occlusion. An inclined bite plane can be useful following functional appliance therapy, either as part of a retainer or as an adjunct during the transition from fixed to functional appliances to help to maintain sagittal correction.
Distal movement of buccal segments
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


