Introduction
The purpose of this study was to evaluate the alveolar bone dimensional changes with cone-beam computed tomography after space-opening procedures for an endosseous implant in patients with unilateral or bilateral maxillary lateral incisor agenesis.
Methods
A pilot retrospective cohort study was conducted of 11 patients (13 sites) in whom the canines had erupted less than 2 mm distally to the central incisors. Pretreatment and posttreatment scans obtained from 3 private practice offices were evaluated for changes in alveolar bone width, height, and labial concavity. A fiducial line representing the ideal location of the longitudinal axis of an endosseous dental implant was used as a reference for the spatial location of the alveolar bone at the lateral incisor site in reference to the adjacent tooth roots at posttreatment. The posttreatment width and height measurements scans were compared with normative data from the contralateral incisor in patients with unilateral agenesis (n = 6).
Results
Alveolar bone width was significantly decreased on average from 17% to 25% along the height of the ridge (2-10 mm) ( P <0.05). The labial concavity was significantly increased compared with the initial dimensions ( P <0.05). No significant changes were found in alveolar bone ridge height.
Conclusions
Significant alveolar bone width decreases and increases in labial concavity were found after implant ridge development in patients with maxillary lateral incisor agenesis. The alveolar bone ridge was located more lingually than the adjacent teeth, suggesting a need for bone grafting to achieve proper fixture placement.
Dental implants are commonly used to replace congenitally missing maxillary lateral incisors once skeletal maturity has been reached. The restorative treatment for these patients is often challenging for the surgeon and the restorative dentist because the 3-dimensional (3D) morphology of the alveolar ridge might be less than ideal. Inadequate alveolar bone width can require surgical bone augmentation to ensure ideal implant positioning and adequate thread coverage. An alternative to grafting is the development of the alveolar ridge through orthodontic movement of an adjacent tooth through the deficient dentoalveolar site.
Ridge development procedures aimed to achieve adequate alveolar ridge dimensions have been reported to be successful when the maxillary canine erupts adjacent to the central incisor and thereafter is distalized with orthodontics to its proper location. As the root of the canine is displaced distally, new bone is deposited, establishing adequate buccolingual width and vertical height of the edentulous ridge site. A recent study found that the ridge of the maxillary lateral incisor is well preserved in the short and long terms, with insignificant clinical losses in width and height, right after alveolar ridge development is completed. However, conflicting results were found in another study that measured bone volume in the lateral incisor site in the short and long terms. A significant volume deficiency was observed immediately after ridge development in the site of the missing lateral incisor. Similarly, another recent study also reported 13% to 15% ridge width decreases in patients when the canine was distalized after erupting close to the central incisor (<2 mm). Furthermore, the authors of this study found that the labial concavity of the alveolar ridge in the lateral incisor site was on average 1.5 mm deep after the canine was distalized.
These conflicting results might be related to varied measurement techniques, which were not consistent in all the studies. Furthermore, all these studies used stone models to evaluate ridge changes that do not reflect the exact underlying alveolar bone changes, which are of primary interest when considering an implant fixture placement. Thus, the objective of this study was to evaluate the alveolar bone dimensional changes with cone-beam computed tomography (CBCT) in patients with unilateral or bilateral maxillary lateral incisor agenesis when the canines erupted less than 2 mm distally to the central incisors. The null hypothesis was that there are no significant dimensional alveolar bone changes in the lateral incisor site after distalization of a canine that erupted close to the central incisor.
Material and methods
This study was a retrospective evaluation of patient records. The study aim and protocols were reviewed, and institutional board approval was obtained from the University of Connecticut (IRB number 11-030-1) before the study.
A pilot retrospective CBCT cohort study was conducted to measure the changes in the maxillary alveolar bone dimensions in patients with lateral incisor agenesis where orthodontic ridge development was done through distalization of the adjacent canine. These patients’ CBCT scans were obtained from 3 private orthodontic offices (Dr Paul Rigali, Wallingford, Conn; and Dr Carl Roy, Virginia Beach and Chesapeake, Va) that routinely use this type of 3D imaging for diagnostic purposes.
The inclusion criteria were unilaterally or bilaterally congenitally missing maxillary lateral incisors, mesially erupted permanent canines adjacent to the central incisors, space between the distal surface of the central incisor and the mesial surface of the canine less than 2 mm, a maxillary canine orthodontically distalized to create space for an endosseous dental implant in the lateral incisor site, no systemic health problems, good periodontal health, and a posttreatment CBCT scan. The exclusion criteria included presence of a deciduous lateral incisor, an impacted or unerupted permanent canine, cleft palate or any other dentofacial deformity, and a history of periodontal disease.
Over 10,000 patient records were screened from the 3 offices, and 60 records of patients with unilateral or bilateral maxillary lateral incisor agenesis were obtained that included a posttreatment CBCT scan taken within 2 months of appliance removal. Among these 60 patients, only 19 had an endosseous dental implant restoration as part of the treatment plan. Finally, only 11 patients’ records met the strict inclusion criteria delineated by this study. The final sample comprised 7 male and 4 female subjects with mean ages of 16.45 ± 5.76 years (range, 11.3-28 yeas) at the beginning of treatment and 18.68 ± 5.79 years (range, 13.6-30.3 years) at the end of treatment ( Table I ). Orthodontic treatment lasted on average 2.4 ± 0.6 years.
| Characteristic | Value |
|---|---|
| Sex | |
| Male | 7 |
| Female | 4 |
| Age and SD (y) | |
| T1 mean | 16.45 ± 5.76 |
| Range | 11.3-28 |
| T2 mean | 18.68 ± 5.79 |
| Range | 13.6-30.3 |
| Sites | |
| Total number of sites | 13 |
| Number of patients with unilateral agenesis | 6 |
| Total sites meeting inclusion criteria | 6 |
| Number of patients with bilateral agenesis | 5 |
| Total sites meeting inclusion criteria | 7 |
| Distribution of sites in patients with bilateral agenesis | 2 patients × 2 sites = 4 sites 3 patients × 1 site = 3 sites |
Three-dimensional CBCT scans were previously obtained using an i-CAT Classic scanner (Imaging Sciences International, Hatfield, Pa). Each scan was acquired with a 20-second scan time with a 16-cm (diameter) × 13-cm (height) field of view at a resolution of 0.3-mm voxels. All images were collected at 120 kV(p) and 3-8 mA. Raw data were reconstructed and exported as 12-bit depth DICOM files using Xoran (i-CAT software, version 2.1.22). The DICOM files were imported into Dolphin 3D (version 11; Dolphin Imaging and Management Solutions, Chatsworth, Calif) for further analysis. The CBCT scans were taken at 2 times, before orthodontic treatment (T1) and at the end of orthodontic treatment (T2). All offices had the same CBCT unit and used the same method to acquire the scans.
Two methods were used to evaluate the alveolar bone width changes at the maxillary lateral incisor site on the CBCT scans. The first method was used to evaluate the alveolar bone widths at T1 and T2. The second method was used to evaluate the available labial and palatal bone to a fiducial line representing the longitudinal axis of an ideal location of an endosseous dental implant in the lateral incisor site at T2 only.
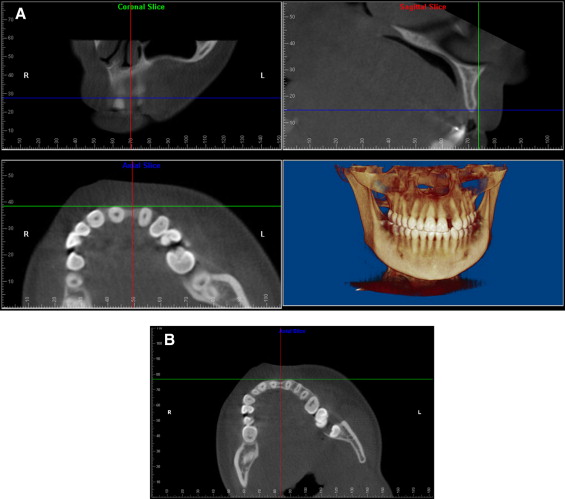
In method 1, the scans were oriented after drawing a line that bisected the angle formed by the longitudinal axes of the maxillary canine and the central incisor mesiodistally and buccolingually. Alveolar bone width measurements were made along the sagittal reference plane at 2, 4, 6, 8, and 10 mm apically to the alveolar bone crest. Additionally, alveolar width measurements parallel to this sagittal plane were made at the same heights apically to the cementoenamel junction at the middle of the central incisor and the canine ( Fig 1 ).
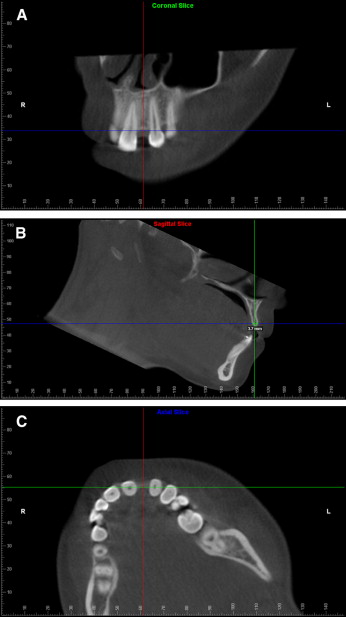
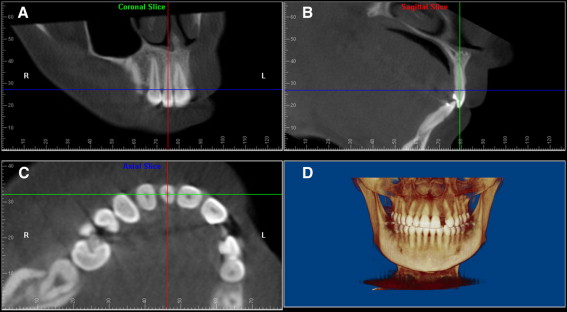
For the second method, 2 lines were used for orientation of the scans. The first line bisected the angle formed by the longitudinal axes of the adjacent maxillary central incisor and the canine mesiodistally. Another line perpendicular to this reference line and tangent to the anterior contours of the pulp canals of the central incisor and canine was drawn. Alveolar width measurements, palatal and labial to this fiducial line at 2, 4, 6, 8, and 10 mm from the alveolar bone crest were measured in the sagittal plane ( Fig 2 ). This method was only used to evaluate the scans at T2. This fiducial line was based on the average location of the longitudinal axis of a maxillary lateral incisor ( Fig 3 ).
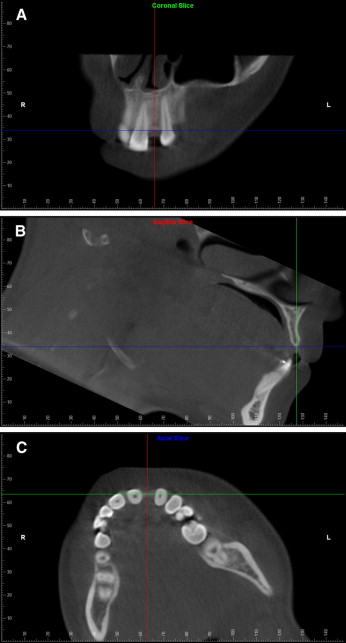
Two methods were used to evaluate alveolar bone height changes. In method 1, the scans were oriented after drawing a line that bisected the angle formed by the longitudinal axes of the maxillary canine and the central incisor mesiodistally and buccolingually. A line connecting the incisal edges of the canine and the central incisor (best fit), perpendicular to these lines, was used to measure the height of the alveolar bone crest. Measurements were taken from this line to the alveolar bone crest on the coronal slice: (1) distally to the central incisor, (2) at the middle of the ridge, and (3) mesially to the canine ( Fig 4 ). For method 2, the same reference lines for method 1 were used. A reference line connecting the cementoenamel junctions of the maxillary canine and the central incisor (best fit), on the coronal slice, was used to measure the changes in alveolar bone height on the middle of the ridge ( Fig 5 ).
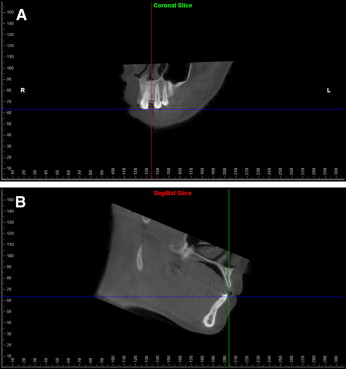
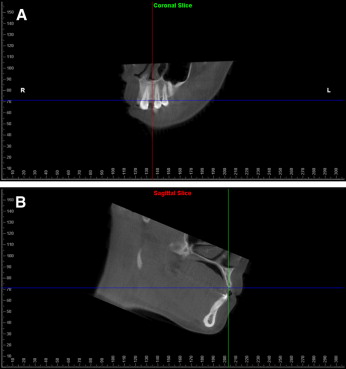
The changes in the labial concavity were evaluated by orienting the scans with a line that bisected the angle formed by the longitudinal axes of the maxillary canine and the central incisor mesiodistally and buccolingually. The distance from the deepest concavity observed between the central incisor and the canine to a reference line tangent to the most prominent labial aspect of these 2 teeth was recorded at 2, 4, 6, 8, and 10 mm apically to the alveolar crest in the axial slice ( Fig 6 ).
Incisor inclination changes as a result of space opening were evaluated by measuring the angulation of the central incisor to the palatal plane. In addition, all measurements of alveolar bone width and labial concavity where the maxillary lateral incisor was present (control side) in patients with unilateral agenesis (n = 6) were compared with the contralateral developed alveolar sites at T2.
Statistical analysis
T1 and T2 scans were collected from 11 patients with unilateral or bilateral lateral incisor agenesis. Measurements were taken in the sites with lateral incisor agenesis and in the contralateral side in patients with unilateral agenesis. A total of 13 sites in these 11 patients were examined, and the unit of analysis was each site. Measurements were made by the same examiner (S.P.). Data were imported into SPSS software (version 20; SPSS, Chicago, Ill) for analysis. Means, standard deviations, and 25%, 50% (median), and 75% quintiles were reported for all T1 and T2 variables. Because of the small sample size and because the data were not normally distributed, nonparametric tests were used to compared outcomes. A Wilcoxon signed rank test was used to analyze T1 and T2 differences for the treatment side, and to compare the posttreatment changes with the control side in patients with unilateral agenesis. All statistical tests were 2-sided, and a P value of <0.05 was deemed statistically significant.
All variables were remeasured to assess measurement error and reliability. Intrarater reliability was estimated using the Cronbach alpha coefficient.
Results
The Cronbach alpha for double measurements for the selected data points ranged from 0.65 (T2 bone width at 2 mm in the middle of the ridge) to 0.99 ( Table II ). On the treatment sites, the space for the lateral incisor was opened to a width of 6.63 ± 1.24 mm from an average space of 0.95 ± 0.74 mm at T1. This final space dimension was similar to the contralateral incisor in patients with unilateral agenesis, where the mesiodistal width was 6.78 ± 0.86 mm. The space was opened through distalization of the canine and labial tipping of the incisor reflected by an increase of the incisor’s inclination to the palatal plane by an average of 6.43° ( P <0.05) ( Table III ). Alveolar bone height changes were not significant for either measurement method with treatment.
| Outcome | Cronbach alpha | |
|---|---|---|
| T1 | T2 | |
| Space between incisor and canine | 0.96 | 0.87 |
| Height method 1 (mesial crest) | 0.93 | 0.86 |
| Height method 1 (middle crest) | 0.96 | 0.81 |
| Height method 1 (distal crest) | 0.96 | 0.82 |
| Height method 2 | 0.87 | 0.68 |
| Bone width at 2 mm central incisor | 0.82 | 0.77 |
| Bone width at 4 mm central incisor | 0.86 | 0.90 |
| Bone width at 6 mm central incisor | 0.95 | 0.96 |
| Bone width at 8 mm central incisor | 0.94 | 0.97 |
| Bone width at 10 mm central incisor | 0.82 | 0.84 |
| Bone width at 2 mm middle ridge | 0.84 | 0.65 |
| Bone width at 4 mm middle ridge | 0.97 | 0.69 |
| Bone width at 6 mm middle ridge | 0.99 | 0.95 |
| Bone width at 8 mm middle ridge | 0.98 | 0.93 |
| Bone width at 10 mm middle ridge | 0.96 | 0.97 |
| Bone width at 2 mm canine | 0.92 | 0.90 |
| Bone width at 4 mm canine | 0.97 | 0.88 |
| Bone width at 6 mm canine | 0.98 | 0.94 |
| Bone width at 8 mm canine | 0.99 | 0.93 |
| Bone width at 10 mm canine | 0.99 | 0.97 |
| Labial concavity at 2 mm | 0.87 | 0.92 |
| Labial concavity at 4 mm | 0.75 | 0.93 |
| Labial concavity at 6 mm | 0.91 | 0.93 |
| Labial concavity at 8 mm | 0.90 | 0.78 |
| Labial concavity at 10 mm | 0.87 | 0.73 |
| Incisor inclination | 0.90 | 0.96 |
| Palatal bone width at 2 mm | — | 0.97 |
| Palatal bone width at 4 mm | — | 0.98 |
| Palatal bone width at 6 mm | — | 0.97 |
| Palatal bone width at 8 mm | — | 0.97 |
| Palatal bone width at 10 mm | — | 0.97 |
| Labial bone width at 2 mm | — | 0.68 |
| Labial bone width at 4 mm | — | 0.68 |
| Labial bone width at 6 mm | — | 0.73 |
| Labial bone width at 8 mm | — | 0.83 |
| Labial bone width at 10 mm | — | 0.80 |
| Outcome | Pretreatment | Posttreatment | Posttreatment – pretreatment | P value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Percentile distribution | Mean | SD | Percentile distribution | Mean difference | ||||||
| 25th | 50th | 75th | 25th | 50th | 75th | |||||||
| Space between incisor and canine | 0.95 | 0.74 | 0 | 1.10 | 1.65 | 6.63 | 1.24 | 5.45 | 6.80 | 7.30 | 5.68 | 0.001 † |
| Height method 1 (mesial crest) | 8.48 | 0.94 | 7.95 | 8.10 | 8.75 | 8.18 | 1.28 | 7.40 | 8.30 | 9.20 | −.30 | 0.420 |
| Height method 1 (middle crest) | 8.50 | 0.97 | 8.00 | 8.30 | 8.70 | 8.44 | 1.68 | 7.55 | 8.50 | 9.45 | −.06 | 0.834 |
| Height method 1 (distal crest) | 8.55 | 1.23 | 7.90 | 8.20 | 8.75 | 8.25 | 1.52 | 7.70 | 8.20 | 9.15 | −.30 | 0.439 |
| Height method 2 | 1.41 | 0.91 | 0.55 | 1.20 | 2.15 | 1.32 | 0.90 | 0.60 | 1.30 | 2.05 | −.09 | 0.624 |
| Bone width at 2 mm central incisor | 7.05 | 0.59 | 6.55 | 7.00 | 7.55 | 6.60 | 0.52 | 6.30 | 6.60 | 6.85 | −.45 | 0.031 ∗ |
| Bone width at 4 mm central incisor | 7.42 | 0.78 | 6.75 | 7.20 | 8.05 | 6.87 | 0.77 | 6.35 | 6.60 | 7.25 | −.55 | 0.006 † |
| Bone width at 6 mm central incisor | 7.46 | 1.02 | 6.55 | 7.20 | 8.35 | 6.58 | 1.22 | 5.90 | 6.20 | 7.20 | −.88 | 0.012 ∗ |
| Bone width at 8 mm central incisor | 7.69 | 1.17 | 7.00 | 7.40 | 7.95 | 6.34 | 1.27 | 5.45 | 6.00 | 6.95 | −1.35 | 0.006 † |
| Bone width at 10 mm central incisor | 8.24 | 1.75 | 6.80 | 7.70 | 10.40 | 6.95 | 1.52 | 5.70 | 7.20 | 7.40 | −1.29 | 0.036 ∗ |
| Bone width at 2 mm middle ridge | 5.55 | 2.01 | 4.85 | 5.70 | 7.10 | 4.58 | 1.02 | 3.95 | 4.60 | 5.05 | −.97 | 0.046 ∗ |
| Bone width at 4 mm middle ridge | 6.82 | 1.28 | 5.70 | 7.00 | 7.85 | 5.31 | 1.05 | 4.45 | 4.90 | 6.05 | −1.51 | 0.001 † |
| Bone width at 6 mm middle ridge | 6.84 | 1.71 | 5.45 | 6.50 | 8.30 | 5.48 | 1.42 | 4.65 | 5.40 | 5.95 | −1.36 | 0.002 † |
| Bone width at 8 mm middle ridge | 6.78 | 1.84 | 5.45 | 6.20 | 7.85 | 5.42 | 1.84 | 4.55 | 5.50 | 6.30 | −1.36 | 0.003 † |
| Bone width at 10 mm middle ridge | 7.34 | 2.04 | 5.65 | 6.80 | 8.55 | 5.68 | 1.93 | 4.60 | 5.50 | 6.50 | −1.66 | 0.002 † |
| Bone width at 2 mm canine | 8.42 | 1.12 | 7.40 | 8.60 | 8.90 | 7.62 | 1.23 | 7.00 | 7.70 | 8.40 | −.80 | 0.017 ∗ |
| Bone width at 4 mm canine | 8.89 | 1.17 | 8.20 | 8.50 | 9.70 | 8.22 | 1.09 | 7.35 | 8.10 | 9.05 | –.67 | 0.002 † |
| Bone width at 6 mm canine | 8.64 | 1.46 | 7.65 | 8.20 | 9.90 | 8.35 | 0.89 | 7.60 | 8.50 | 9.20 | −.29 | 0.53 |
| Bone width at 8 mm canine | 8.39 | 1.60 | 7.35 | 8.00 | 9.85 | 8.38 | 1.19 | 7.40 | 8.60 | 9.25 | −.01 | 0.875 |
| Bone width at 10 mm canine | 8.39 | 1.69 | 7.10 | 7.70 | 9.80 | 8.32 | 1.47 | 7.30 | 8.50 | 9.30 | −.07 | 0.727 |
| Labial concavity at 2 mm | 0.3 | 0.48 | 0 | 0 | 0.85 | 0.84 | 0.83 | 0 | 1.00 | 1.35 | .54 | 0.011 ∗ |
| Labial concavity at 4 mm | 0.68 | 0.61 | 0 | 1.10 | 1.20 | 1.05 | 0.83 | 0.25 | 1.10 | 1.45 | .37 | 0.058 |
| Labial concavity at 6 mm | 0.97 | 0.63 | 0.30 | 1.10 | 1.45 | 1.39 | 0.81 | 1.00 | 1.50 | 1.85 | .42 | 0.016 ∗ |
| Labial concavity at 8 mm | 1.13 | 0.67 | 0.65 | 1.20 | 1.65 | 1.58 | 0.77 | 1.05 | 1.90 | 2.10 | .45 | 0.028 ∗ |
| Labial concavity at 10 mm | 0.87 | 0.54 | 0.60 | 0.80 | 1.30 | 1.22 | 0.68 | 0.80 | 1.40 | 1.70 | .35 | 0.049 ∗ |
| Incisor inclination | 110.71 | 6.91 | 107.3 | 109.0 | 117.4 | 117.14 | 8.28 | 110.0 | 116.0 | 123.5 | 6.43 | 0.010 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


