Introduction
In this study, we evaluated the reliability and validity of 3 bite registrations in relation to condylar position in the glenoid fossae using magnetic resonance imaging in a symptom-free population.
Methods
Nineteen subjects, 14 men and 5 women (ages, 20-39 years) without temporomandibular disorders were examined. Three bite registrations were taken and evaluated on each subject: centric occlusion, centric relation, and Roth power centric relation. The differences in condyle position among the 3 bite registrations were determined for the left and right condyles: centric occlusion-centric relation, centric occlusion-Roth power centric relation, and centric relation-Roth power centric relation for each plane of space.
Results
The results indicated that (1) all measurements collected had large standard deviations and ranges with no statistical significance, and (2) of the 19 subjects and 38 condyles assessed, 33 condyles (87%) were concentric in an anteroposterior plane. In the transverse anatomic plane, all condyles were concentric.
Conclusions
The clinical concept of positioning the condyles in specific positions in the fossae with various bite registrations as a preventive measure for temporomandibular disorders and as a diagnosis and treatment planning tool is not supported by this study.
The relationship among condylar position, occlusion, and temporomandibular disorders (TMD) has been the subject of much debate in dentistry for more than a century. A significant part of the debate involves establishing coincidence between a specific definition of centric relation and centric occlusion. It is believed by many gnathologists and the like that failure to achieve this position will predispose patients to developing TMD in the future.
Despite the lack of data available to support this assertion, many dentists continue to persist in marrying a particular definition of centric relation with centric occlusion as a main goal of treatment. With the current emphasis in dentistry on evidence-based decision-making, the routine establishment of centric occlusion with centric relation in all patients is subject to question.
Centric relation is defined as a position of the condyles in the glenoid fossae, irrespective of the occlusion or tooth contact. Centric occlusion is an interocclusal dental position of the maxillary teeth relative to the mandibular teeth. Over the past half century, the definition of centric relation has evolved from a posterior position of the condyle in relation to the glenoid fossa to a posterosuperior position to eventually an anterior and superior position. Before 1968, centric relation was considered to be a retruded (posterior) condylar position. The latest edition of the Glossary of Prosthodontic Terms defines centric relation as “a maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterosuperior position against the slopes of the articular eminences.”
Contemporary orthodontic gnathologists believe in attaining an anterosuperior condyle position at the same time the teeth are in centric occlusion (centric relation equals centric occlusion); however, there is little or no scientific evidence to support this view. Dentists who believe in establishing a coincidence of a specific definition of centric relation with centric occlusion unnecessarily subject their patients to procedures that might include orthodontics and irreversible bite-altering procedures, leading to significant financial and biological costs to their patients. In fact, the evidence supports the contrary notion. According to Alexander et al, magnetic resonance imaging (MRI) data of the temporomandibular joint showed that condyles are not located in the assumed positions as advocated by certain centric bite registrations such as retruded centric relation and leaf-gauge generated centric relation registrations. Centric bite registrations attempting to locate retruded (posterosuperior) centric relation and contemporary anterosuperior centric relation do not correspond to the condyle positions of people without TMD. The location of the condyles in the glenoid fossa, irrespective of position, has not been demonstrated to be consequential to the presence or absence of TMD symptoms.
The Roth power centric relation is perhaps the most commonly used contemporary gnathologic record aimed at attaining an anterosuperior centric relation position. To date, MRI has not verified the actual anatomic position of the condyles when this bite registration is taken. The condylar positions in centric occlusion and Roth power centric relation have only been studied on articulators with mandibular or condylar position indicators. The validity of this approach has been questioned and is not supported by MRI data, presumably the most accurate ionizing radiation-free means of assessing 3-dimensional condyle-disc-fossa relationships. In this study, condylar position was assessed using MRI after the use of 3 common bite registrations: centric occlusion, retruded centric relation, and the so-called Roth power centric relation.
Material and methods
Ethics approval for this study was obtained from the Human Research Ethics Committee at the University of Western Australia. Guided by a power analysis, a sample of 19 subjects was studied.
The subjects were 14 men and 5 women (ages, 20-39 years) who met the following criteria: (1) permanent dentition, (2) no congenital craniofacial anomaly or syndrome, (3) no skeletal asymmetry or premature tooth contacts leading to any functional mandibular displacements, (4) no history of trauma to the face or jaws, (5) positive overjet and overbite, (6) no TMD signs or symptoms (all subjects underwent a TMD examination based on the Research Diagnostic Criteria for TMD; although clicking without other symptoms does not indicate pathosis or dysfunction, subjects with clicking were excluded from the study ), and (8) completed an MRI safety screening check.
Each participant was also informed of the risk of finding any incidental pathology after the MRI scan, but no significant incidental pathology was found.
To standardize the bite registration technique, all records were taken by the same investigator (S.K.). Three bite positions were assessed. The first was centric occlusion, with the subject biting together in maximum intercuspation.
The remaining 2 bite registrations were taken in wax (blue wax; Delar, Lake Oswego, Ore).
Retruded centric relation was taken by applying distal pressure to the chin and taking a wax record at the first point of light occlusal contact. All subjects exhibited a discrepancy between centric relation and centric occlusion. By taking a record at the first point of light occlusal contact, we were able to establish a reference point to base our repeated measurements. This proved to be a highly reproducible registration technique in this study.
Roth power centric relation was taken with a 2-piece wax registration consisting of anterior and posterior sections. The anterior section was first constructed at a vertical where the posterior teeth are at least 2 mm apart. This piece of wax was chilled and allowed to harden. This wax was then placed back into the mouth, a softened posterior section was placed, and the patient was instructed to bite. The mandibular anterior teeth were guided into the hardened anterior section of wax without a slide into the indentations. As the patient closed into the hardened anterior section, he or she was instructed to “close firmly and hold.” The posterior section was chilled with air. When the posterior section had hardened sufficiently to prevent distortion, both wax sections were removed and chilled.
Once the hard wax bite registrations were obtained, they were used to position the subjects’ mandibles in the various occlusal positions as the MRI data were obtained. Originally, acrylic records of the bite positions were fabricated after the articulation of plaster, with the assumption that they would be more accurate. We found, however, that these acrylic records distorted significantly during the fabrication process and provided an inaccurate reflection of the bite records. Since the changes in the bite positions were small, this would have significantly affected the results. We then decided to use the hard wax records, which were stable and more accurate.
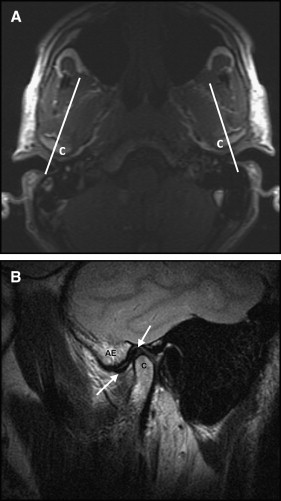
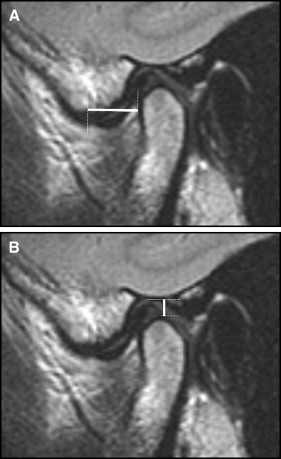
MRI scans of each subject were acquired as the subjects occluded at each of the 3 bite relationships. All scans were performed on the same MRI scanner (1.5 T, Signa Excite; General Electric, Fairfield, Conn). Scans were performed with dedicated phased array surface temporomandibular joint coils. An initial low-resolution T1-weighted (repetition time [TR]: 340 ms; echo time [TE], 8 ms) axial localizing scan was followed by a high-resolution T2-weighted (TR 2800 ms, TE 72 ms) sagittal oblique scan acquired perpendicular to the long axis of each condyle ( Fig 1 ). The MRI scans were interpreted by a head and neck radiologist (R.B.) with 8 years of experience reading MRIs of the temporomandibular joint. He was blinded as to which bite registration he was assessing in each subject, and the order of scanning was randomized by the MRI technician. On each side and in each position, measurements of the anteroposterior and superoinferior positions of the condyle with respect to the temporal bone were measured using the following standard cortical bony landmarks: for the anteroposterior position, the anterior margin of the condyle and the summit of the articular eminence; for the superoinferior position, the highest point of the condyle and the deepest concavity of the glenoid fossa ( Fig 2 ).
From the sagittal and transverse anatomic plane MRI views, the radiologist evaluated the concentricity of the left and right condyles in the glenoid fossa in the centric occlusion position. This was done by dividing the condyle into thirds and determining which third was within the central point of the glenoid fossa.
Guided by a power analysis, the 19 subjects were studied to produce 80% power to detect mean differences of at least 1 mm at the 0.05% level of significance.
To assess the variability and reproducibility associated with taking the centric occlusion, centric relation, and Roth power centric relation bite registrations, 3 sets of each were recorded on 3 separate occasions on 2 subjects. These readings were analyzed by a 1-way repeated-measures analysis of variance (ANOVA), which showed no significant ( P <0.05) difference between the repeated positions, an indication that this method of determining centric occlusion, centric relation, and Roth power centric relation is reliable.
One observer (the radiologist, R.B.) made all measurements, 3 times on 2 randomly chosen subjects with a 1-week interval between measurements. Intraclass correlation coefficients (ICC) were used to determine the intraobserver reliability, and 95% prediction limits for the errors in measurement are provided. A mean ICC of 0.992 was determined, with an upper limit of 0.995 and a lower limit of 0.985.
Statistical analysis
For both the left and right condyles, the differences in condyle position among the 3 bite registrations were determined: centric occlusion-centric relation, centric occlusion-Roth power centric relation, and centric relation-Roth power centric relation for each plane of space. The data were analyzed by 1-way ANOVA and by randomized block 1-way ANOVA with Tukey follow-ups.
Results
For both the left and right condyles, the differences in condyle position between the different bite registrations were determined as follows: centric occlusion-centric relation, centric occlusion-Roth power centric relation, and centric relation-Roth power centric relation for each plane. The results are presented in the Table .


