Introduction
Orthodontists assess mesiodistal root angulations before, during, and after orthodontic treatment as an aid in establishing proper root position. Panoramic imaging has been useful for this purpose and is a valuable screening tool in diagnosis and planning treatment of orthodontic patients. Cone-beam computed tomography (CBCT) for imaging of the craniofacial complex creates the opportunity to evaluate 3-dimensional images compared with traditional 2-dimensional images. The purpose of this project was to compare mesiodistal root angulations by using posttreatment panoramic radiographic images and CBCT scans.
Methods
Mesiodistal root angulations from panoramic images and CBCT scans of 35 orthognathic surgery patients after orthodontic treatment were compared. The panoramic images were measured by using VixWin (Gendex Dental Systems, Des Plaines, Ill), and the CBCT scans by using InvivoDental 3D (version 4.1, Anatomage, San Jose, Calif). The mesiodistal root angulation of each maxillary and mandibular tooth was measured by using the occlusal plane as the reference line. With an intercept-only linear regression for correlated data (with an unstructured covariance structure), the global test of whether the mean vector of all differences for the teeth is zero was performed separately for the 2 arches.
Results
The global test for both arches was statistically significant ( P <0.001), indicating an overall difference in root angulation between measurements from panoramic and CBCT images. There was no discernible pattern in the average differences between panoramic and CBCT measurements.
Conclusions
The assessment of mesiodistal tooth angulation with panoramic radiography should be approached with caution and reinforced by a thorough clinical examination of the dentition.
During orthodontic treatment, the alignment of the roots of the teeth in parallel axial inclinations is critical for the correct alignment and occlusion of the teeth and for maintaining a stable orthodontic result. Panoramic radiographs have traditionally been used as a diagnostic aid before, during, and after orthodontic treatment to assess root position. The clinical examination portion of the American Board of Orthodontics certification requires the submission of panoramic radiographs for documentation of root inclination and parallelism after treatment.
Unfortunately, because panoramic image generation necessitates large beam deviations from the perpendicular to the object and film, tooth position and inclination can be distorted or magnified by varying amounts during acquisition. Numerous investigators have evaluated angular distortion in panoramic images, especially with regard to tooth inclination. These investigations have demonstrated that panoramic images have limits when used for the assessment of mesiodistal angulations. Angular distortion in the radiograph results from the combined variable distortions in the horizontal and vertical dimensions. The angulations measured from panoramic images relative to known angulations have demonstrated significant alterations in the mesiodistal angulations for most maxillary and mandibular teeth.
Cone-beam computed tomography (CBCT) of the craniofacial complex provides the opportunity to evaluate patient anatomy, including the occlusion and tooth angulations, in 3 dimensions. Peck et al used CBCT for comparison with panoramic images before orthodontic treatment in 5 subjects. The angulations measured from the panoramic images were different from those based on CBCT reconstructed panoramic images, and the standard panoramic images produced a false impression of mesial tilt on the maxillary anterior teeth and distal tilt on the maxillary posterior teeth, but there was no recognizable pattern in the mandible. The conclusion was that the values from CBCT reconstructed panoramic images were more accurate because CBCT reconstructions do not have the distortions inherent in 2-dimensional panoramic radiograph acquisitions. The purpose of this project was to compare the mesiodistal root angulations measured from posttreatment panoramic radiographic images and CBCT volumes, rather than from reconstructed panoramic images. Study participants had completed orthodontic treatment and orthognathic surgery and received concurrent panoramic radiographs and NewTom CBCT (3G, AFP Imaging, Elmsford, NY) scans after the postsurgical orthodontic phase of treatment (approximately 1 year after surgery).
Material and methods
Study subjects were obtained from a review of the clinical records of 155 subjects who had consented to participate in an ongoing prospective observational project (NIH grant DE 05215, “influences on stability following orthognathic surgery”), approved by the Biomedical Institutional Review Board, between July 21, 2003, and May 1, 2008. Each subject signed a consent form (assent with parental permission) and a HIPAA consent for the use of clinical records. The inclusion criteria were concurrent panoramic and CBCT images taken after the postsurgical phase of orthodontic treatment (approximately 1 year after surgery) and a panoramic radiograph obtained by using the Orthophos XG Plus (Sirona Dental Systems, Charlotte, NC). Subjects were excluded if they had at least 1 dilacerated root per quadrant because of the difficulty in determining the long axis of the tooth, or if more than 1 tooth per quadrant anterior to the first molar was missing.
Each subject was assigned a random identification number so that the examiner (D.G.B.) would be masked to the subject when measuring the panoramic radiographs and the CBCT scans. Panoramic images were captured via a charge-coupled device image sensor and imported to the VixWin (Gendex Dental Systems, Des Plaines, Ill) software package for measurement ( Fig 1 ). CBCT scans were obtained in DICOM (digital imaging and communications in medicine) format by using the NewTom 3G and were accessed by using InvivoDental 3D (version 4.1, Anatomage, San Jose, Calif) imaging software to allow measurements ( Fig 2 ).
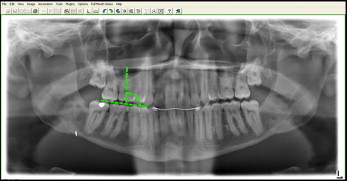

Mesiodistal root angulations were measured from the first molar anteriorly for all teeth. All measurements were made by using the occlusal plane as the reference line. The occlusal plane was constructed in the panoramic image by connecting the cusp tips of all teeth and in the CBCT volume by orienting the occlusal plane parallel to the lower border of the display window from the sagittal and coronal views. The long axis of the tooth was determined to complete each angular measurement relative to the occlusal plane. In the CBCT volume and panoramic radiograph, the long axis of the tooth was defined by the buccal cusp tip or midpoint of the incisal edge and the root apex for single-rooted teeth, and the occlusal aspect of the buccal groove and the depth of the bifurcation or trifurcation for multi-rooted teeth. In the CBCT volume, custom sections were created from the axial slice, and each measurement was made from a facial view of the tooth in the posterior. For the CBCT measurements of the anterior teeth, the volume rendering was reoriented to view the tooth from the facial aspect, and a custom section was created from the sagittal slice before measurement of the tooth.
Ten subjects were randomly selected. The measurement procedures (importing the images and making measurements) were repeated with 1 week between the initial and the replicate measurements. Reliability and systematic bias were assessed separately for the panoramic and CBCT images by using intraclass correlation statistics and paired t tests, respectively.
Statistical analysis
To assess the differences in mesiodistal root angulations between the panoramic images and the CBCT scans, an intercept-only linear regression for correlated data, accounting for the correlation in each subject, with an unstructured covariance was fit separately for the maxillary and mandibular arches. These models examined whether the differences between the CBCT scans and the panoramic images were nonzero, and, if so, whether the differences were related to tooth location.
Results
The clinical records of 155 subjects who had consented to participate in an ongoing prospective observational project between July 21, 2003, and May 1, 2008, were reviewed; 118 subjects were imaged with a panoramic machine other than the Orthophos XG Plus, and 2 subjects were excluded due to several missing teeth or dilacerated roots in 1 quadrant, resulting in 35 subjects in the sample. Approximately 54% of the subjects were female, and 83% were white, with an average age of 21.2 ± 6.5 years.
The intraclass correlation coefficients ranged from 0.98 to 1.0 for the measurements obtained from the panoramic radiographs and from 0.99 to 1.0 for the CBCT measurements, indicating excellent intraobserver reliability. No mean difference for the replicate CBCT measurements was statistically significant ( P >0.05). The mean differences for the replicate panoramic angulations for maxillary right canine and first molar and left lateral incisor were statistically significantly different ( P <0.05) from zero; the replicate measurements tended to be slightly greater than the first set; however, no mean difference was greater than 0.5°.
The mean differences between the panoramic and the CBCT angulations for both arches were statistically significant ( P <0.0001). There was no clear pattern for the differences in either arch ( Tables I and II ), although the differences between the panoramic and CBCT angulations were statistically significantly different for all maxillary anterior teeth. There were statistically significant differences in mesiodistal tooth angulations for 75% of maxillary and 67% of mandibular teeth.
| Panoramic | CBCT | Pan-CBCT ∗ | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Tooth | n | Mean | SD | Mean | SD | Mean | SD | Estimate | P value |
| Right | |||||||||
| First molar | 35 | 94.1 | 5.4 | 92.3 | 4.7 | 1.74 | 5.27 | 1.74 | 0.06 |
| Second premolar | 35 | 93.8 | 6.4 | 93.6 | 5.9 | 0.20 | 4.32 | 0.20 | 0.79 |
| First premolar | 23 | 95.5 | 5.5 | 95.1 | 4.0 | 0.43 | 4.41 | 1.34 | 0.13 |
| Canine | 35 | 87.7 | 6.7 | 97.7 | 6.2 | −10.03 | 6.87 | −10.03 | <0.001 |
| Lateral incisor | 34 | 83.4 | 3.8 | 89.2 | 5.9 | −5.79 | 5.12 | −5.71 | <0.001 |
| Central incisor | 35 | 89.5 | 3.2 | 88.0 | 3.0 | 1.46 | 2.54 | 1.46 | 0.002 |
| Left | |||||||||
| Central incisor | 35 | 91.7 | 3.0 | 88.9 | 3.6 | 2.86 | 3.17 | 2.86 | <0.001 |
| Lateral incisor | 34 | 86.2 | 4.4 | 90.1 | 4.3 | −3.85 | 3.90 | −3.79 | <0.001 |
| Canine | 35 | 90.5 | 5.9 | 99.6 | 6.6 | −9.03 | 5.49 | −9.03 | <0.001 |
| First premolar | 23 | 100.5 | 4.7 | 98.9 | 2.7 | 1.61 | 4.24 | 2.10 | 0.03 |
| Second premolar | 35 | 97.3 | 6.2 | 95.1 | 5.1 | 2.23 | 4.33 | 2.23 | 0.004 |
| First molar | 35 | 93.6 | 4.7 | 95.2 | 3.4 | −1.60 | 3.78 | −1.60 | 0.02 |
∗ Pan-CBCT values: positive values indicate greater distal inclination on the panoramic image relative to the CBCT volume, and negative values indicate greater mesial inclination on the panoramic image relative to the CBCT volume.
| Panoramic | CBCT | Pan-CBCT ∗ | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Tooth | n | Mean | SD | Mean | SD | Mean | SD | Estimate | P value |
| Right | |||||||||
| First molar | 35 | 97.8 | 5.9 | 93.5 | 3.1 | 4.29 | 5.72 | 4.29 | <0.001 |
| Second premolar | 35 | 92.3 | 5.6 | 92.5 | 5.5 | −0.23 | 6.01 | −0.23 | 0.82 |
| First premolar | 26 | 88.4 | 5.4 | 91.7 | 5.1 | −3.12 | 5.19 | −3.30 | 0.01 |
| Canine | 35 | 100.2 | 6.7 | 99.3 | 4.9 | 0.83 | 5.28 | 0.83 | 0.36 |
| Lateral incisor | 35 | 92.6 | 7.0 | 86.9 | 5.0 | 5.63 | 5.39 | 5.63 | <0.001 |
| Central incisor | 34 | 89.4 | 4.5 | 88.6 | 3.0 | 0.82 | 3.75 | 1.01 | 0.13 |
| Left | |||||||||
| Central incisor | 34 | 90.9 | 5.1 | 87.6 | 2.7 | 3.35 | 4.83 | 3.13 | 0.001 |
| Lateral incisor | 35 | 93.2 | 7.0 | 85.8 | 4.2 | 7.37 | 6.56 | 7.37 | <0.001 |
| Canine | 35 | 99.9 | 6.7 | 97.2 | 5.0 | 2.66 | 6.82 | 2.65 | 0.03 |
| First premolar | 27 | 87.2 | 7.0 | 91.5 | 5.4 | −4.26 | 6.37 | −5.08 | <0.001 |
| Second premolar | 35 | 91.7 | 6.6 | 91.9 | 4.4 | −0.23 | 5.72 | −0.23 | 0.81 |
| First molar | 35 | 97.0 | 5.3 | 93.6 | 3.9 | 3.40 | 4.55 | 3.40 | <0.001 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


