Introduction
The objective of this research was to evaluate commercially available preformed archwire forms compared with normal dental arch forms.
Methods
Thirty mandibular dental casts were made of orthodontically untreated subjects with the most ideal occlusions, selected from among approximately 3500 students at Nippon Dental University. Canine and first-molar widths were measured on the dental casts with a 3-dimensional laser scanning system. Twenty preformed mandibular archwires were scanned by using a flatbed scanner. The archwire widths were measured at the level of the mean canine and first-molar depths, and then compared with the natural dental arch widths, considering bracket thickness, measured with a modified caliper. The results were statistically analyzed with the Mann-Whitney test.
Results
The preformed archwires that most closely matched the normal dental arch forms were the Orthos (Ormco, Glendora, Calif) and Vari-Simplex large (Ormco) types. The preformed archwires were significantly narrower than the normal dental arches at both the canine ( P <0.05) and molar ( P <0.01) levels.
Conclusions
The variations in current preformed archwires do not correspond entirely with various arch forms in a group with ideal occlusion. The most commonly used archwires are similar and can be considered imitations of the Roth arch form, which was designed primarily for extraction patients in the 1970s. Therefore, preformed archwires that are approximately 1 to 3 mm wider at the canine level and 2 to 5 mm wider at the first-molar level might be required for today’s orthodontic needs.
The invention of the edgewise appliance in the late 1920s brought about the consideration of the relationship between the dental arch form of a normal occlusion as a goal of orthodontic treatment on the one hand and the archwire form of orthodontic appliances on the other. In 1934, Chuck stated, “With edgewise arch appliance, arch form becomes the basis of our treatment planning, because in the use of the appliance we predetermine the arch form and create an ideal archwire to which we move the teeth.” The classic Bonwill-Hawley type of preformed stainless steel archwire blanks were introduced to improve the efficacy of orthodontic treatment. When the preadjusted edgewise appliance was introduced in the 1970s, preformed archwire blanks for this new system also became available. This new preformed archwire, designed by Andrews based on his extensive research on nonorthodontic normal occlusion and the clinical experience of Roth, met with great success. With the spread of this appliance, a variety of archwire forms have been developed for various reasons.
To date, little research has been conducted on the rationale behind the prefabricated archwire form. Most studies in this area sought stable orthodontic results, and their findings have not varied. For example, Felton et al compared 10 kinds of archwires with the dental arch forms of 30 subjects with untreated normal occlusions selected from the 120-patient sample of Andrews. They successfully classified all 30 dental arch forms into 10 archwire shapes and reported that 27% of the subjects fit the Vari-Simplex form from Ormco, and 20% were close to the Tru-Arch form from Ormco/“A” Company. On the other hand, Braun et al analyzed 16 popular nickel-titanium (NiTi) archwires and compared them with the mean shape of the dental arch. They reported that all sampled strong-selling, preformed archwires were wider than the normal dental arch form.
Therefore, it is necessary to study preformed archwire forms to increase the efficacy of tooth movement and to achieve stability of orthodontic treatment. The purpose of this study was to evaluate whether the various commercially available orthodontic archwire forms are comparable with the diversity of natural normal dental arch forms.
Material and methods
From a total population of approximately 3500 students at Nippon Dental University, 30 orthodontically untreated subjects (15 men, 15 women; mean age, 23 years 2 months) were clinically examined according to the following inclusion criteria: no history of orthodontic treatment; Angle Class I molar relationship with arch form symmetry and minimal arch-length discrepancy; complete dentition, excluding third molars; ideal overjet and overbite; no prosthetic crowns and minimal restorations; minimal signs of occlusal attrition; and balanced facial esthetics (no significant discrepancies noted). About 100 sets of dental casts were then made, and the most ideal Class I occlusions were selected for analysis. The mandibular arch was analyzed for this study, because therapeutic possibilities in the mandible are more limited than in the maxilla, the maxillary arch form is strongly associated with the mandible, and also maintaining mandibular canine width is an essential element in achieving stable orthodontic treatment results.
Eight kinds of brackets for the central incisor, canine, and first molar with 0.022-in slots from 7 manufacturers were selected to obtain the mean bracket base thickness ( Table I ).
| Bracket | Manufacturer |
|---|---|
| MiniTwin | Ormco/“A” Company, Orange, Calif |
| Mini Diamond | Ormco, Glendora, Calif |
| Mini Master | American Orthodontics, Sheboygan, Wis |
| Elite Opti-MIM | Ortho Organizers, San Marcos, Calif |
| MicroArch | GAC International, Bohemia, NY |
| Victory | 3M Unitek, Monrovia, Calif |
| Metal Bracket | Dentsply, Sankin, Japan |
| NU Edge-LN | TP Orthodontics, LaPorte, Ind |
Twenty kinds of preformed NiTi archwires from 8 manufacturers were selected for analysis ( Table II ). Although we evaluated NiTi archwires, each manufacturer also produces preformed stainless steel archwires identical in design to the NiTi archwires.
| Archwire form | Manufacturer |
|---|---|
| Accu Form | GAC International, Bohemia, NY |
| Broad Arch (large) | Ormco, Glendora, Calif |
| Broad Arch (small) | Ormco, Glendora, Calif |
| Natural Arch Form I | American Orthodontics, Sheboygan, Wis |
| Natural Arch Form II | American Orthodontics, Sheboygan, Wis |
| Natural Arch Form III | American Orthodontics, Sheboygan, Wis |
| Ortho Form I | 3M Unitek, Monrovia, Calif |
| Ortho Form II | 3M Unitek, Monrovia, Calif |
| Ortho Form III | 3M Unitek, Monrovia, Calif |
| Orthos (large) | Ormco, Glendora, Calif |
| Orthos (small) | Ormco, Glendora, Calif |
| Pro Form | Ortho Organizers, San Marcos, Calif |
| Smooth Arch Form | Oral Care, Tokyo, Japan |
| Standard Form | GAC International, Bohemia, NY |
| Tru-Arch (medium) | Ormco/“A” Company, Orange, Calif |
| Tru-Arch II (medium) | Ormco/“A” Company, Orange, Calif |
| Tynilloy (large) | Dentsply-Sankin, Tokyo, Japan |
| Tynilloy (small) | Dentsply-Sankin, Tokyo, Japan |
| Vari-Simplex (large) | Ormco, Glendora, Calif |
| Vari-Simplex (small) | Ormco, Glendora, Calif |
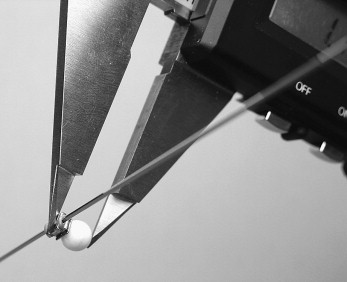
Mean bracket thicknesses were used for the distance between the facial axis point (FA point) and the bracket slot point (BS point). A ceramic sphere (diameter, 4.75 mm) was attached to 1 tip of a digital caliper (Digimatic caliper, NTD12-15C, Mitutoyo, Kawasaki, Japan) to fit the curvature of the bracket base. Brackets were then tied with elastic ligatures to a 0.0215 × 0.028-in stainless steel wire. The distances between the center of the bracket mesh base and the base of the bracket slots for the central incisor, canine, and molar were measured by the modified caliper in 0.01 mm resolution ( Fig 1 ).
The means and standard deviations of bracket thicknesses at the mandibular central incisor, canine, and first molar were 1.34 ± 0.16, 0.75 ± 0.11, and 0.73 ± 0.08 mm, respectively.
Thirty mandibular dental casts were scanned and analyzed by using a noncontact 3-dimensional orthodontic cast measuring system (Surflacer VMS-250R, UNISN, Osaka, Japan). The FA point for 14 teeth (from both sides of the central incisors to the second molars) were plotted on the surface of a cloud data set from a 3-dimensionally digitized mandibular dental cast according to the original anatomic definition of the points. In addition, the 30 sets of 14 x- and y-coordinates of the FA points for each dental arch were analyzed by using Excel 2000 (Microsoft, Redmond, Wash).
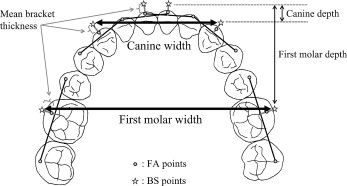
The BS point represents the position of the base of the bracket slot in relation to the tooth. The positions of the BS points on the labial and buccal sides of the teeth were defined by first connecting a line between the FA points on the 2 adjacent teeth on both sides of the tooth of interest. A line perpendicular to this axis was then extended so that it passed through the FA point on the tooth of interest. The BS points were then established at the outward distance of the mean bracket thickness from the corresponding FA point ( Fig 2 ). An axis was extended between the BS points on the central incisors, and a reference point was established on the axis halfway between the BS points. This midpoint served as the point of reference from which the depths of the canine and the first molar could be measured ( Fig 2 ). The means and standard deviations of the canine and the first-molar depths of the 30 normal subjects were 5.09 ± 0.70 and 26.95 ± 1.56 mm, respectively.
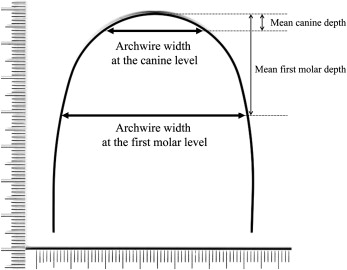
The 20 kinds of archwires were scanned with millimeter gauges by using a flatbed scanner (ES-2000, Epson, Suwa, Japan) at a resolution of 600 dpi (23.6 dots per mm) ( Fig 3 ) by using image-editing software (version 7.0, Photoshop, Adobe, San Jose, Calif). The images were then analyzed by using image processing and analysis software (Scion Image, National Institutes of Health, Bethesda, Md). The points on the lingual surface at which the archwire and the line parallel to the line connecting the distal ends of the wire intersected with the level of the mean canine and first-molar depths were digitized. The distance between the bilateral intersection points at the canine and first-molar levels was calculated as the width of the archwire. The means and standard deviations of the archwire widths at the canine and first-molar levels of 20 preformed archwires were calculated and statistically analyzed.
The absolute error of the FA point identification on dental casts with the 3D scanning system we used was less than 0.08 mm.
All sample archwires were measured twice in randomized order more than 2 months later. The measurement error was evaluated according to Dahlberg’s formula. The errors of the method of measurement on the scanned images of archwires were 0.04 mm for canine width and 0.02 mm for molar width. The means of the 2 repeated measurements were used for the analysis.
Statistical analysis
Means and standard deviations; median, lower (first) quartile, 25th percentile (Q1), and upper (third) quartile,75th percentile (Q3); and the differences in the median values of the arch widths were calculated. The nonparametric Mann-Whitney test was used to analyze the average differences in canine and first-molar widths at the 5% and 1% levels. A nonparametric test was used for this study because the distributions of archwire widths among the 20 commercial products did not fit normal distribution. Additionally, the distributions of preformed archwire widths at the canine and first-molar levels were graphically compared with means and standard deviations of normal dental arch widths, because the distribution of natural dental arch widths is usually considered normal distribution.
Results
Table III shows the means and standard deviations, medians, maximums, and Q1 and Q3 values of the canine and first-molar widths of the 30 normal subjects and the 20 preformed archwires. Statistically significant differences between the subjects and the archwires were observed for the widths of both canine and first molar (canine width: U = 188.5, P = 0.0272; molar width: U = 92.0, P <0.0001 [U is the calculation of a statistic in a non-parametric Mann-Whitney test, given by the formula: U = R-n(n+1)/2, where n is the total number of observations, and R is the sum of the ranks in the sample]).
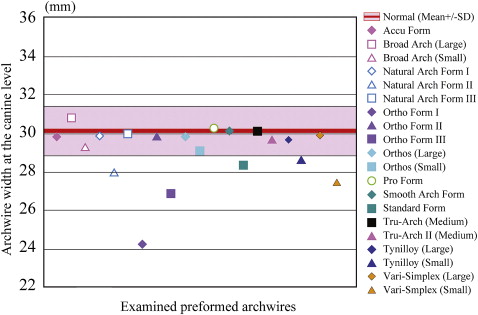
Figure 4 shows the distribution of widths at the canine level of the 20 archwires compared with the means and standard deviations of the normal dental arch width, and Figure 5 shows the distribution of the widths at the first-molar level. Fourteen of the 20 archwires had widths at the canine level within 1 SD of the mean for the normal sample. In contrast, only 7 archwires were within 1 SD of the mean for normal first-molar width.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


