Introduction
The purpose of this study was to clarify the frontal chewing patterns of various crossbite malocclusions.
Methods
A mandibular kinesiograph was used to record the masticatory movements of 106 subjects (ages, 12-35 years) with crossbite malocclusion and 22 subjects (ages, 16-30 years) with normal occlusion. The chewing patterns were classified into 8 chewing types according to the cycle shape of the frontal incisor point movement. The crossbite subjects were divided into 5 groups by the anteroposterior position of the crossbite, and then the subjects with posterior crossbite were divided into 3 groups by the transverse position of the crossbite. The Mann-Whitney U test was used to compare the frequency of each chewing type between any crossbite group and the control group; and between the various crossbite groups.
Results
In the crossbite groups, normal chewing occurred much less often than in subjects with normal occlusion. In the posterior crossbite group, reverse chewing was greater ( P = 0.002), and normal chewing was less frequent ( P = 0.001) compared with the anterior crossbite group. When accompanied by mandibular shift, mandibular prognathism, arch crossbite, in the crossbite or shift side, reverse type, and reverse-crossing type occurred more often than in contralateral side.
Conclusions
In the frontal plane, patients with posterior crossbite might have more abnormal chewing types than those with anterior crossbite, and posterior crossbite could contribute to the high frequency of reverse and reverse-crossing chewing types, especially when accompanied by mandibular shift, mandibular prognathism, or arch crossbite.
Crossbite, either anterior or posterior, is a common malocclusion that has been reported to be associated with abnormal function of the masticatory muscles and signs and symptoms of temporomandibular disorders (TMD). It is important to know whether crossbite has a specific effect on masticatory movement, especially the cycle shape of incisal point movements on the frontal plane (frontal chewing patterns).
Ahlgren established a morphologic classification of frontal chewing patterns; however, the relationship between chewing patterns and malocclusion type including crossbite was not found, even after analyzing the chewing types of 290 subjects with malocclusion and 30 with normal occlusion. Although the chewing patterns of crossbite malocclusion (especially posterior crossbite) have been investigated by others, the results were inconsistent. Some studies found that reverse, cross, chopping, or other abnormal chewing types had higher frequencies in posterior crossbite or crossbite patients. In addition, Pröschel and Hofmann found a different chewing pattern distribution in subjects with mandibular prognathism compared with Class I and Class II Division 2 patients, but no difference was found in any parameter studied during the masticatory cycle between the unilateral posterior crossbite group and the normal group in the study of Martin et al.
The inconsistency of the results could be assigned to the differences in sample selection and methods for measurement and analysis. For example, the ages of the samples were different, including mixed dentition, early permanent dentition, adults, or mixed dentition to early permanent dentition, and so on. Studies of chewing patterns of normal occlusion have shown that the typical chewing patterns of subjects aged 12 to 14—characterized by sagittal opening and wide lateral closing movements—had changed completely compared with patterns in the deciduous and mixed dentitions. Hence, it might be more reasonable to analyze the effect of occlusion on chewing patterns of subjects in the same age range. Moreover, some authors noticed that some TMD patients had different chewing patterns, but it was unclear in the selected subjects with or without TMD features in some previous studies. Probably, this was another reason that caused the inconsistent, and even controversial, results.
The purposes of this study were to analyze the frontal chewing patterns in patients (aged 12-35 years) with various crossbite malocclusions without signs and symptoms of TMD and then to study the effect of different positions of crossbite on chewing patterns in the anteroposterior and transverse directions.
Material and methods
The sample for this study comprised 106 subjects with crossbite malocclusion (ages, 12-35 years; 70 female, 36 male) and 22 subjects with normal occlusion (ages, 16-30 years; 15 female, 7 male; dental and skeletal Class I relationship according to molar relationship, ANB angle, and convexity; less than 3 mm of crowding and less than 3 mm of anterior overjet and overbite). The malocclusion subjects were selected from a consecutive group of 917 patients visiting the First Orthodontic Department, Tokyo Medical and Dental University. We checked their data, including pretreatment casts, clinical examination records, questionnaire data and raw pretreatment mandibular kinesiograph recordings. Subjects with normal occlusion were chosen from nursing students and dental postgraduate and graduate students in this university. In the entrance criteria established for this study, subjects with crossbite and normal occlusion were excluded if they had clinical signs and symptoms of TMD according to clinical examination and questionnaire, a history of orthodontic treatment, extensive restorations, cast restorations, pathologic periodontal conditions, or missing teeth. Subjects with functional crossbites were excluded by clinical examinations in this study. For patients with posterior crossbite, the presence or absence of mandibular shift and or mandibular prognathism was not an entrance criterion. All subjects were informed and agreed to participate in this study. Ethics approval was given by this university before the start of this research. First, all patients with crossbite were divided into 5 groups according to the anteroposterior position of crossbite.
Group 1 included those with only individual anterior crossbite, without posterior crossbite; group 2, those with at least 4 anterior teeth in crossbite, without posterior crossbite; group 3, those with continuous anterior and posterior crossbites (eg, arch crossbite involving 1 side); group 4, those with individual posterior crossbite, without anterior crossbite; and group 5, similar to groups 1 and 2, but with individual posterior crossbite simultaneously.
Then the patients with posterior crossbite (groups 3-5) were divided into 3 groups according to the transverse position of crossbite: group A, left posterior crossbite; group B, right posterior crossbite; and group C, bilateral posterior crossbite.
The distribution of malocclusion details of groups A through C is shown in Table I , considering the possible effect of mandibular shift, mandibular prognathism, position of the teeth in crossbite, individual posterior crossbite, or posterior crossbite involving more than 2 teeth of 1 side or bilateral arch (arch crossbite) on the chewing patterns of subject with posterior crossbite.
| Right crossbite, n (%) | Left crossbite, n (%) | Bilateral crossbite, n (%) | ||
|---|---|---|---|---|
| 1 | Individual crossbite | 8 (53.3) | 20 (95.2) | 4 (21.1) |
| Arch crossbite | 7 (46.7) | 1 (4.8) | 15 (79.9) | |
| 2 | Only premolar | 1 (6.7) | 4 (19.0) | 3 (15.8) |
| First molar involved | 11 (73.3) | 10 (47.6) | 15 (78.9) | |
| Only second or third molar | 3 (20) | 7 (33.3) | 1 (5.3) | |
| 3 | Right shift | 7 (46.7) | 0 (0) | 1 (5.3) |
| Left shift | 0 (0) | 6 (28.6) | 8 (42.1) | |
| No shift | 8 (53.3) | 15 (71.4) | 10 (52.6) | |
| 4 | Mandibular prognathism | 8 (53.3) | 4 (19.0) | 15 (78.9) |
| No mandibular prognathism | 7 (46.7) | 17 (71) | 4 (11.1) |
Pretreatment masticatory movements of the patients and the subjects with normal occlusion were recorded with a mandibular kinesiograph system (K6-I cranio-mandibular evaluation system, Myotronics-Noro Med, Seattle, Wash). This system allow 3-dimentional recording of mandibular movements without interfering with the motion of the jaw. The masticatory recordings of all subjects were done by 2 examiners (Q.N. and Z.K.), who carefully complied with the manufacturer’s protocol. The masticatory movements of 5 randomly selected patients were examined twice by the same examiners; statistical tests showed no significant difference for the results of mandibular kinesiograph recordings between the 2 times (linear parameters, maximum opening, maximum lateral displacement, Student t test, P >0.05; the distribution of chewing types described in the next paragraph and the statistical analysis, Mann-Whitney U test, P >0.05). Similar tests were performed between the 2 examiners for 5 other randomly selected patients, with similar results. The accuracy and reliability of the mandibular kinesiograph meets the needs of a clinical study as the study of Keeling et al demonstrated.
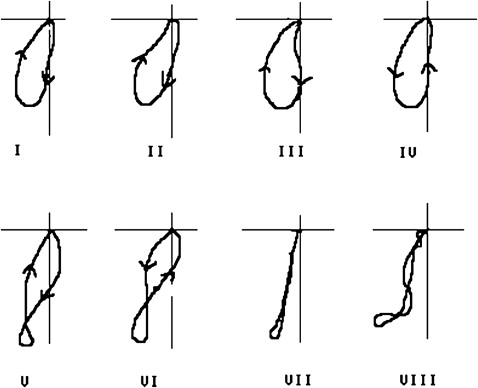
Chewing gum was selected as the experimental food because it could form a more consistent bolus than natural food to produce a consistent masticatory pattern over many cycles, and its size and solidity were stable during mastication so that the occlusal condition was easily reflected by chewing. Before we recorded the masticatory movements, the subjects were instructed to chew the gum until it was sufficiently soft. Then, free chewing, right-side chewing, and left-side chewing were recorded. For chewing on either side, 10 strokes, from the fifth to the 14th, were analyzed because they had the least variability in both path and rhythm. The chewing type of each stroke was classified by visual examination according to the cycle shape of incisor point movement on the frontal plane as shown in the Figure . The chewing types were as follows.
- I.
Normal: smooth opening toward the working side and smooth convex closing. This often occurred in normal occlusion including types I and III in the classifications of Akiyama et al.
- II.
Concave closing: opening similar to I, but concave closing.
- III.
Concave opening: closing similar to I, but concave opening.
- IV.
Reverse: shape similar to I, but opening and closing directions were contrary to I.
- V.
Positive crossing: opening and closing paths were crossed; in the occlusal phase, the directions of opening and closing were the same as I.
- VI.
Reverse crossing: opening and closing paths were crossed, but, in the occlusal phase, the directions of opening and closing were the same as IV.
- VII.
Superimposition: the closing path almost superposes with the opening path.
- VIII.
Irregular: opening and closing movements with no consistent pattern and frequent crossing of the opening and closing phases.
Statistical analysis
Contingency statistics (chi-square test) were used to compare the distribution of malocclusion manifestations between the right, left, and bilateral posterior groups. The level of significance was set at 0.05.
The number of strokes of each chewing type in the 10 strokes in either side was counted and considered as the frequency of each chewing type in either side. The average of the number of strokes in the right and left sides was used to represent unilateral chewing. The Mann-Whitney U test (a nonparametric test) was used to compare the frequency of each chewing type in the 10 strokes between the crossbite and normal occlusion groups, between the crossbite groups (including comparisons of crossbite groups 1 to 5, and between the anterior and posterior crossbite groups), and between the crossbite and contralateral sides for patients with posterior crossbite. The level of significance was set at 0.05.
Results
The distribution of malocclusion manifestations of the right, left, and bilateral posterior crossbite groups is shown in Table I . The position distribution of the crossbite teeth in each group was similar, but the ratios of arch crossbite and mandibular prognathism were higher in the right and bilateral posterior groups than in the left posterior crossbite group ( P = 0.003 and P = 0.000 for arch crossbite; P = 0.031 and P = 0.001for mandibular prognathism, respectively). For the percentage of shift, the ratio of right shift in the right group was not significantly different from that of left shift in the left group, and the distribution of shifts in the bilateral crossbite group was similar to that of the left group ( P >0.05).
Table II shows the frequency of each chewing type in different anteroposterior positions of the crossbite groups. In all crossbite groups, type I occurred significantly less often than in normal occlusion. In addition, groups 3, 4, and 5 had higher frequencies of type IV than in normal occlusion ( P <0.01 or P <0.001). Moreover, group 4 (individual posterior crossbite) had a higher frequency of reverse-crossing chewing and superimposition types than in normal occlusion. Comparisons between any 2 crossbite groups showed no significant difference for the frequency of any chewing type between groups 1 and 2 ( P >0.05) and between groups 3, 4, and 5 ( P >0.05). In addition, groups 1 and 2 had anterior crossbite without posterior crossbite. Groups 3, 4, and 5 included patients with posterior crossbite; thus, groups 1 and 2 were combined as the anterior crossbite group, and groups 3, 4, and 5 were combined as the posterior crossbite group.
| Group | Subjects (n) | Means of the numbers of each chewing type in the 10 strokes | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | VII | VIII | |||
| 1 | 37 | Mean | 5.76 † | .54 | .76 | .90 | .61 | 1.11 | .23 | .09 |
| SD | 3.39 | 1.37 | 1.43 | 1.57 | 1.19 | 1.92 | .49 | .31 | ||
| 2 | 14 | Mean | 6.82 † | .36 | .07 | .64 | 1.22 ∗ | .43 | .47 | .00 |
| SD | 2.56 | .93 | .27 | .95 | 1.48 | 0.94 | 1.05 | .00 | ||
| 3 | 25 | Mean | 3.78 ‡ | 1.12 ∗ | .38 | 2.00 ‡ | 1.00 | 1.36 | .26 | .10 |
| SD | 2.95 | 1.93 | 1.10 | 1.92 | 1.45 | 2.38 | .54 | .29 | ||
| 4 | 16 | Mean | 3.91 ‡ | .31 | .97 | 1.94 ‡ | .19 | 1.28 ∗ | 1.38 † | .03 |
| SD | 3.36 | 1.25 | 2.11 | 2.50 | .36 | 1.63 | 2.75 | .13 | ||
| 5 | 14 | Mean | 4.82 ‡ | .18 | .86 | 1.89 † | .57 | 1.21 | .43 | .04 |
| SD | 2.93 | .67 | 1.68 | 2.38 | .76 | 1.72 | .78 | .13 | ||
| Normal occlusion | 22 | Mean | 8.84 | .09 | 0.34 | .09 | .34 | .33 | .07 | .00 |
| SD | 1.23 | 0.25 | 0.89 | 0.20 | 0.58 | 0.46 | 0.15 | 0.00 | ||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


