Fig. 2.1
Preoperative orthopantomography: 3.8 is impacted and dysodontiasic (arrow); restorative treatment in tooth 4.7, partially edentulous dental arches

Fig. 2.2
Preoperative panorex CBCT
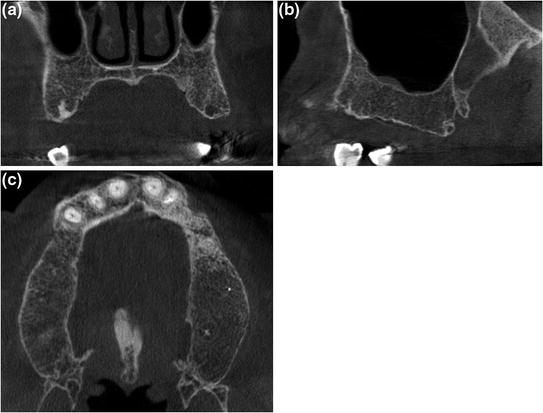
Fig. 2.3
Preoperative CBCT: coronal (a), sagittal (b) and axial (c) scans showing partially edentulous maxilla
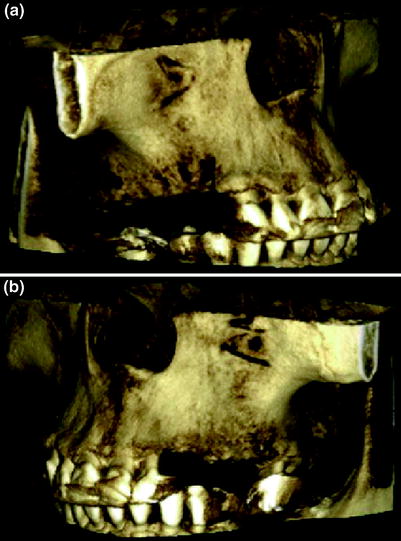
Fig. 2.4
Preoperative CBCT: 3D reconstruction of right (a) and left (b) edentulous maxillary emiarch

Fig. 2.5
Posttreatment extraoral photographs (a, b, c): frontal and lateral views of upper and lower arches

Fig. 2.6
Post-treatment orthopantomography: implant screws are placed correctly in the site of 1.4, 1.5, 1.6, 2.3, 2.5, 2.6
Preoperative CBCT examination with accurate volumetric images allows for a precise evaluation of paranasal sinuses anatomy and an estimation of buccal and palatal bone volume in the surgical interest area.
2.2 Dental Anomalies
Dental anomalies represent a very extensive subject which include number anomalies (hyperodontia, hypodontia), volume anomalies (macrodontia, microdontia), shape anomalies (dental fusions, root variations), structural anomalies (hereditary and acquired), and position anomalies (dysodontiasis, ectopic and heterotopic teeth).
The most common anomaly is dysodontiasis that is eruption difficulty due to the lack of appropriate space within dental arch or the teeth wrong orientation.
Dentoalveolar surgery for impacted teeth is very common in dental clinical practice. The third inferior molars, followed by superior canines, central superior incisors, inferior canines, first and second superior premolars, are the most frequently involved teeth in abnormal eruption. Even deciduous teeth could present with dysodontiasis diseases.
Generally eruption defects cause tooth entrapment in correspondence of the alveolar fossa, sometimes it could determine an ectopic location at the level of the palatine bone, of the chin or of other deeper bony regions. For example, most of the times the third inferior molar (most frequently affected by dysodontiasis) has a mesial orientation, with its crown close to the second molar’s roots; less commonly it results impacted onto the mandibular rising branch.
Radiological imaging is very important not only to confirm the presence of impacted teeth but also to evaluate their precise position, their location in respect to the occlusal plane, their orientation (position of the tooth long axis compared with adjacent teeth long axis), and their relationship with surrounding anatomical structures, allowing for an accurate presurgical plane.
Conventional 2D radiographs (periapicals, occlusals, panoramics) can be sufficient to identify an impacted tooth, even if the dentist have to perform several radiographs in order to understand the real tooth location administering a significant radiation dose to the patient. Further, plain films often results globally superficial to determine those elements essential for an appropriate presurgical planning.
CBCT technology is particularly indicated for the diagnosis of impacted teeth because it allows for a better analysis of the dental arches: each tooth does not undergo dimensional and perspective alterations, and superimposition of anatomical structures are eliminated with consequent improved definition of bony landmarks, also minimizing measurement errors. The use of 3D reconstructions also allows for a more comprehensive visual picture for the treating dentist to provide proper vectors of tooth movement.
CBCT not only provides precise information on the impacted tooth location, but also allows for an accurate measurement of the distance from adjacent teeth roots; this information is critical for determining the biomechanics treatment plan needed to bring the impacted tooth into the arch without damaging adjacent teeth.
Location of the mandibular canal, in which omonimous nerve and vessels run, and its close contact to the third molar root structures are risk factors in dentoalveolar surgery. However, the mandibular canal, in some cases, may follow a tortuous path, and may not be reliably interpreted on a 2D image.
Multiplanar views obtained from a CBCT are useful not only in tracking the canal, but also in assessing a bifurcated or trifurcated canal. In addition, knowledge of the location of the canal allows the surgeon for establishing a safer surgical plan without complications, related to the access to the tooth and root elevation.
Ankylosis of impacted teeth is another potential complication in dentoalveolar surgery. Plain films are not reliable in revealing ankylosis of teeth.
In conclusion, compared to panoramic radiography, CBCT images allow for better risk assessment of third molar removal and optimization of the surgical times facilitating postsurgical course.
The use of CBCT imaging by now is essential also in planning surgical extraction of impacted maxillary canines as periapical and panoramic radiographs are often inadequate to locate them and to identify their relationship to the roots of the lateral incisors.
In the end, it is essential to highlight that CBCT offers significant advantages even in pediatrics; the acquisition of a small volume in children is sufficient to enclose the whole dental arches and to perfectly localize impacted teeth with dose saving; above all it is possible to minimize the exposure reducing the field of view and performing an examination on a single tooth or a limited group of teeth of clinical concern.
Case
-
41-year-old female.
-
CBCT required for extraction of the mandibular third molars 3.8, 4.8 (Figs. 2.7, 2.8, 2.9, 2.10).
 Fig. 2.7Extraoral photograph: frontal view of upper and lower arches
Fig. 2.7Extraoral photograph: frontal view of upper and lower arches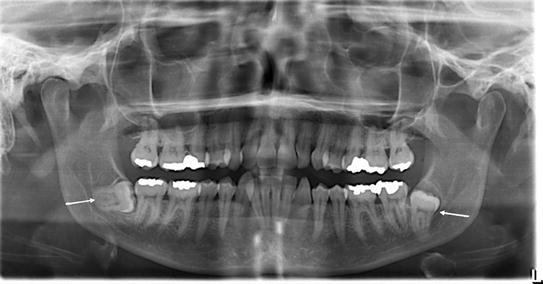 Fig. 2.8Preoperative orthopantomography: restorations in tooth 1.6, 1.7, 2.6, 2.7, 3.6, 3.7, 4.6, 4.7; mandibular third molars are impacted and dysodontiasic (arrows)
Fig. 2.8Preoperative orthopantomography: restorations in tooth 1.6, 1.7, 2.6, 2.7, 3.6, 3.7, 4.6, 4.7; mandibular third molars are impacted and dysodontiasic (arrows)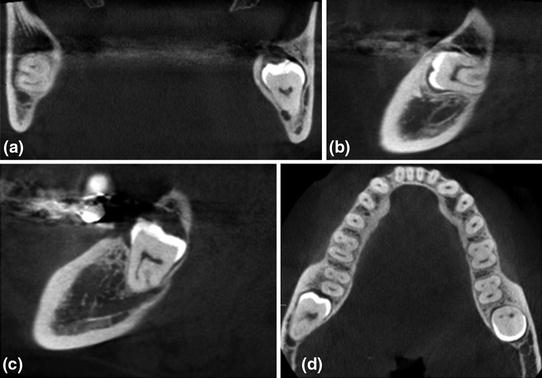 Fig. 2.9CBCT: coronal (a), sagittal (b, c) and axial (d) scans of 3.8, 4.8; mandibular third molars are impacted and dysodontiasic; 4.8 (b) moves mesially and is in relation with the superior wall of the mandibular canal; 3.8 (c) surrounds the vestibular wall of the mandibular canal that is therefore median-palatal to the root of the tooth
Fig. 2.9CBCT: coronal (a), sagittal (b, c) and axial (d) scans of 3.8, 4.8; mandibular third molars are impacted and dysodontiasic; 4.8 (b) moves mesially and is in relation with the superior wall of the mandibular canal; 3.8 (c) surrounds the vestibular wall of the mandibular canal that is therefore median-palatal to the root of the tooth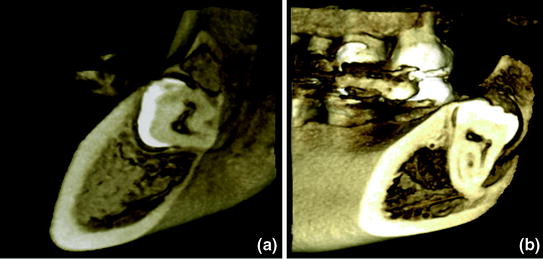 Fig. 2.10CBCT 3D reconstruction of mandibular right (a) and left (b) third molar
Fig. 2.10CBCT 3D reconstruction of mandibular right (a) and left (b) third molar
2.3 Inflammatory and Degenerative Diseases
Inflammatory and degenerative disorders affecting the dental arches can be distinguished, on the basis of their localization, in periodontal (they primarily involve the gums, the alveolar bone, the periodontal ligament and the cementum) and endodontic pathologies (that arise from the dental pulp).
Although clinical diagnosis is essential, in periodontal diseases (both inflammatories and degeneratives) the radiological examination has a central role in the diagnostic and treatment–outcome evaluation of these patients, being capable of detecting, characterizing, and quantifying contingent defects of the adjacent alveolar bone. This may result in rarefaction (in acute inflammatory and degenerative conditions) or sclerosis phenomena (especially in chronic inflammations) or both aspects.
Panoramic and intraoral radiographs often result inadequate in discriminating fine anatomical details that are necessary for a clear visualization of the small structures surrounding the teeth; they also often underestimate the real extent of bone destruction (early lesions could not generate significant radiopacity changes). Furthermore, some bony defects, located on the vestibular or lingual side of the teeth or covered by superimposed structures, can be difficult to interpret with 2D images.
CBCT system has overcome these limitations. Compared to digital- and film-based conventional radiography, it shows significantly higher accuracy in early detection of periodontal bone disorders, which could lead to better treatment outcomes. Multiplanar views provide detailed information on the periodontal conditions, illustrate the location and extension of the bone destruction, differentiating local from generalized forms, and accurately define the possible involvement of the vestibular or lingual cortical plate.
As for periodontal disease, CBCT technology promises to be superior to 2D imaging for the characterization of endodontic pathologies, giving considerable advantages both in diagnostic phase and in posttreatment follow-up.
CBCT imaging achieves a more accurate evaluation of specific morphological features in 3D in comparison to 2D. CBCT provides essential information on:
-
teeth morphology, including pulp chamber size and degree of calcification;
-
location and number of root canals: as the success of endodontic treatments depends on the identification of all root canals (so that they can be accessed, cleaned, shaped, and obturated), the use of CBCT systems is certainly recommended. Unlike conventional radiographic techniques, in which the superimposition of anatomic structures hinders the detection of small components, CBCT is able to identify not only each root canal, but also the possible presence of a second mesiobuccal canal in maxillary first molars;
-
characteristics of periapical lesions: CBCT sensitivity is significantly higher than that of radiographs in detecting periapical osteolytic areas. The high-quality and anatomically detailed CBCT images are unique in the early evaluation of small structural density changes and the differentiation between internal (IRR) and external root resorptions (ERR). Moreover, precisely quantifying IRR and ERR could not be done prior to the introduction of CBCT imaging because of distortion and magnification on 2D radiographs;
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


