This case report describes the orthodontic camouflage treatment for a 16-year-old Chinese girl with a Class III malocclusion. The treatment included extractions of the mandibular second molars, fixed appliance therapy, and miniscrew-aided mandibular arch distalization. Pretreatment, posttreatment, and 2-year follow-up records are shown. The anterior negative overjet and the Class III molar and canine relationships were corrected. The patient’s facial profile was greatly improved. The mandibular third molars erupted into the second molar spaces, with acceptable intercuspation with the maxillary dentition.
Highlights
- •
A patient with a Class III malocclusion was treated.
- •
We extracted the mandibular second molars and distalized the arch with miniscrew anchorage.
- •
The patient’s profile was greatly improved with this treatment modality.
- •
The 2-year follow-up showed a stable occlusion.
The treatment options associated with skeletal Class III problems in the late adolescent and adult dentition often involve surgical intervention or orthodontic camouflage treatment. A skeletal Class III malocclusion usually results from mandibular prognathism, maxillary deficiency, or a combination of both. Surgical intervention can correct the skeletal discrepancy in the sagittal, vertical, and transverse dimensions. In mild and moderate skeletal Class III cases, camouflage treatment can reposition the teeth to disguise the skeletal discrepancy and obtain better occlusion, function, and esthetic results.
In camouflage treatment, an anterior crossbite is corrected by retroclination of the mandibular incisors and proclination of the maxillary incisors. Usually, the mandibular premolars are extracted to relieve crowding, alleviate mandibular incisor protrusion, and correct the molar relationship. Distalization of the mandibular dentition is an alternative to premolar extraction to correct a Class III malocclusion. Retraction of the lower lip follows the distalization of the mandibular incisors. Whether the mandibular incisors are tipped back or retracted with bodily movement significantly affects the morphologic change of the labiomental fold.
It had been difficult to distalize the mandibular dentition before the miniscrew was popularly used in orthodontics. With the help of a miniscrew inserted in the retromolar or premolar region, the mandibular dentition can be successfully distalized to a great extent.
In this case report, miniscrew anchorage was applied to distalize the mandibular dentition to correct the anterior crossbite, establish a Class I molar relationship, and correct the concave profile.
Diagnosis
The patient was a 16-year-old Chinese girl with the chief complaint that her “lower front teeth bite in front of the upper teeth.” By comparing the lateral cephalometric radiographs taken 1 year before and on the day of consultation, no further mandibular growth was expected, and orthodontic treatment was initiated. Her medical and dental histories were noncontributory.
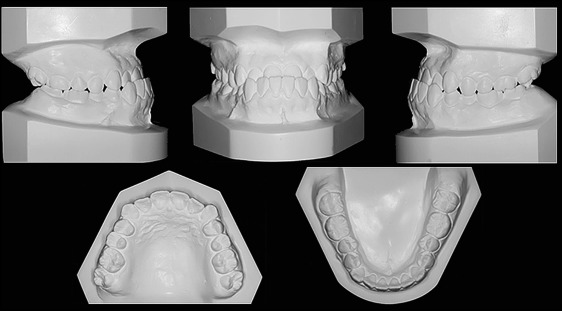
The pretreatment facial photographs showed a mandibular prognathic profile with an acceptable midface convexity and high tension in the labiomental fold. From the front view, no asymmetry was identified. The intraoral photographs showed Class III canine and molar relationships and an anterior crossbite at centric occlusion. Other findings included a deep curve of Spee in the mandibular arch and mild crowding in both arches. The mandible was able to move back slightly with the incisors edge to edge at centric relation ( Figs 1-3 ).


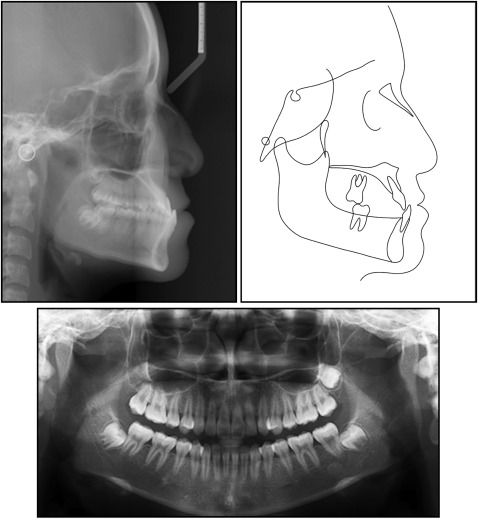
The panoramic radiograph showed a permanent dentition with the maxillary left third molar and mandibular third molars in the forming stage. The mandibular third molars were slightly mesially inclined. The cephalometric analysis showed a skeletal Class III relationship with mandibular prognathism and a slightly decreased mandibular plane angle. The maxillary incisor positions and proclinations were in the normal range in relation to the maxillary palatal plane. The mandibular incisor was slightly retroclined; therefore, the interincisal angle was slightly increased. ( Fig 4 ; Table ). The patient was diagnosed with an Angle Class III malocclusion with mild crowding on a Class III skeletal base with mandibular prognathism in the anteroposterior dimension.
| Pretreatment | Posttreatment | Norm | |
|---|---|---|---|
| Sagittal | |||
| SNA (°) | 85 | 85 | 85 ± 3.5 |
| SNB (°) | 87° | 85.9 | 79 ± 3.0 |
| ANB (°) | −2.0 | −0.9 | 3 ± 2.0 |
| Wits (mm) | −9.7 | −6.5 | −4.5 ± 3.0 |
| Vertical | |||
| Mandibular plane angle (°) | 23.2 | 25.5 | 26.0 ± 4.5 |
| N-ANS (mm) | 52.9 | 53 | 54 |
| ANS-Me (mm) | 59.7 | 62.3 | 64 |
| LFH (%) | 53.02 | 54.03 | 55 |
| Dental | |||
| U1-MxP (°) | 118.6 | 122.8 | 118 ± 6.0 |
| L1-MnP (°) | 92.7 | 86.3 | 97 ± 7.0 |
| U1/L1 (°) | 132.7 | 128.1 | 125 ± 8.0 |
| U1-NA (mm) | 8 | 8.64 | 5 ± 2.0 |
| L1-NB (mm) | 6.76 | 3.56 | 6 ± 2.5 |
| Nasolabial angle (°) | 82 | 80.5 | 110 ± 2.5 |
| Soft tissue | |||
| E-line–lower lip (mm) | 0 | −2.0 | −4.0 ± 4.5 |
Treatment alternatives
Several treatment options were proposed to the patient. First, orthognathic surgery was suggested to set back the mandible; this would lead to a harmonized profile. However, the patient refused the surgical plan for financial reasons and the potential risk.
The second option was orthodontic camouflage treatment with extraction of the premolars. This plan could easily resolve the anterior crossbite, but the mandibular incisors would be tipped back even worse after closing the extraction spaces. With the incisors tipped back, the high tension in the labiomental fold would not be improved. Alternatively, orthodontic camouflage treatment can be carried out with extraction of mandibular molars, usually the third molars. Then the mandibular arch could be distalized with miniscrews to correct the anterior crossbite. In this patient, the mandibular third molars were deeply impacted and close to the inferior alveolar nerve; it would be difficult to surgically remove them. Instead of the third molars, the mandibular second molars could be extracted if the third molars could substitute for the second molars in the long term. The panoramic radiograph showed that the mandibular third molars were forming and slightly mesially inclined. They would possibly erupt into the second molars’ former positions after extraction of the second molars. After discussing this option with the patient, camouflage treatment with extraction of the mandibular second molars was adopted, and consent was obtained from the patient.
Therefore, the treatment plan involved resolving the dental crowding in the maxillary arch by slightly proclining the incisors. In the mandibular arch, the predicted amount of distalization was over 4 mm on both sides. This would help to resolve the crowding, level the curve of Spee, and correct the anterior crossbite.
Treatment progress
After extraction of the mandibular second molars, both arches were bonded and aligned with sequential nickel-titanium wires. Class III elastics (1/4 in, 3.5-oz; Ormco, Orange, Calif) were used for a month on an 0.018-in Australian wire. A miniscrew implant (Orlus 1O16108, 1.6 × 8 mm; Ortholution, Gyeonggi-do, Korea) was inserted in the mandibular buccal shelf region distal to the first molar on each side under local anesthesia. A nickel-titanium coil spring was applied from the miniscrew to distalize the mandibular arch en masse with a continuous force of about 250 g on a 0.0160 × 0.022-in nickel-titanium archwire. The mandibular occlusal plane was rotated counterclockwise because of a moment created by the retraction force ( Fig 5 ). Distalization was discontinued until the molars were overretracted to reach an end-to-end Class II molar relationship. Vertical elastics (3/16 in, 3.5 oz; Ormco) were applied on both sides to correct the open bite in the molar region and the deep anterior overbite. We suggested that the patient should have the maxillary left third molar extracted to align the second molar, but she refused. Then the maxillary molars were intruded to leave enough vertical space for the mandibular third molars to erupt with the help of miniscrews inserted at the palatal side of the maxillary molars (Orlus 1O18309, 1.8 × 9 mm; Ortholution).



