This case report describes the orthodontic treatment of a patient with a deep-overbite Angle Class I malocclusion, agenesis of a mandibular central incisor, and 2 supernumerary teeth, which caused impaction of the mandibular first premolars. The 15-year-old patient also had a convex profile, maxillary dentoalveolar protrusion, and deficiency of space for the correct alignment of teeth. Therefore, treatment consisted of fixed appliance therapy, cervical headgear, extraction of the supernumeraries and the mandibular and maxillary first premolars, and mesiodistal reduction of the maxillary incisors to solve the arch perimeter discrepancy as much as possible with interproximal stripping. This method of treatment significantly improved the patient’s facial and dental esthetics and provided a good functional occlusion, despite the absence of a mandibular incisor, which generally impairs achieving adequate incisal guidance.
Anomaly can be defined as something that deviates from the rule, type, or form. In dentistry, anomalies can involve the number of teeth, such as supernumerary teeth or agenesis of a tooth. Ninety percent to 98% of all supernumerary teeth occur in the maxilla, most commonly in the premaxilla, with an incidence of only 2% to 10% in the mandible. Nevertheless, supernumerary premolars occur most often in the mandible (74%). Supernumerary premolars appear to be more common than previously estimated, occurring 3 times more often in males than in females, and with a greater frequency in the permanent dentition. The most widely accepted theory for the mechanism of supernumerary development is localized hyperactivity of the dental lamina. The occurrence of supernumeraries can create various clinical problems such as derangement of the occlusion, prevention of eruption of adjacent permanent teeth, damage to adjacent teeth, cystic degeneration, and root resorption. Hence, clinical and radiographic evaluation of patients should always be thorough to detect them.
The absence of teeth can also be a challenge to orthodontists. Hypodontia is the congenital absence of at least 1 tooth. The most commonly missing teeth are the third molars, followed by the maxillary lateral incisors and second premolars. The etiology of agenesis might be related to nutritional, traumatic, infectious, hereditary, or phylogenetic factors. Agenesis of canines, maxillary central incisors, and mandibular incisors is relatively rare.
The difficulty of achieving adequate functional occlusion in patients with congenital absence of a mandibular incisor is well known, particularly when the patient has an excessive overbite or overjet and a Bolton tooth-size discrepancy with excess in the mandibular anterior teeth. In these situations, anterior and lateral occlusal guidance will be impaired.
This article presents and discusses the treatment of a patient with Class I malocclusion, with agenesis of a mandibular incisor, deep anterior overbite, excessive overjet, and 2 supernumerary teeth that were blocking the eruption of the mandibular first premolars.
Diagnosis and etiology
A girl, aged 15 years 1 month, had no significant medical history; her chief complaints were spaces between her mandibular teeth and proclined maxillary anterior teeth. Her mother reported no family history of similar malocclusions and mentioned that her daughter had regular dental care. No facial trauma or parafunctional habits were reported. The cause of her malocclusion was presumed to be a combination of genetic and developmental factors.
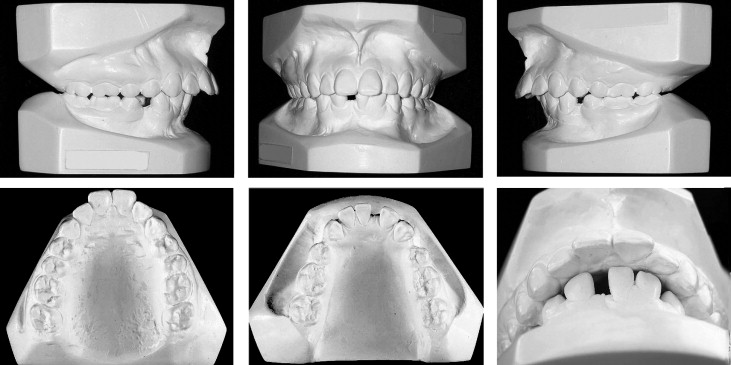
From a frontal view, her face was well balanced and symmetric ( Fig 1 ). Her facial profile was convex, with an acute nasolabial angle, slight mandibular retrusion, strained lip seal, and normal vertical proportions. Intraorally, she had Angle Class I molar and Class II canine relationships on both sides. The maxillary midline was coincident with the facial midline, and both arch forms were ovoid. Her oral hygiene was excellent, with good periodontal health, and all restorations were satisfactory. She was congenitally missing a mandibular central incisor and had 2 nonerupted mandibular first premolars, which were impacted by supernumerary teeth. Overbite was excessive (70%), overjet was 6 mm, and both mandibular and maxillary incisors were proclined ( Fig 2 ).

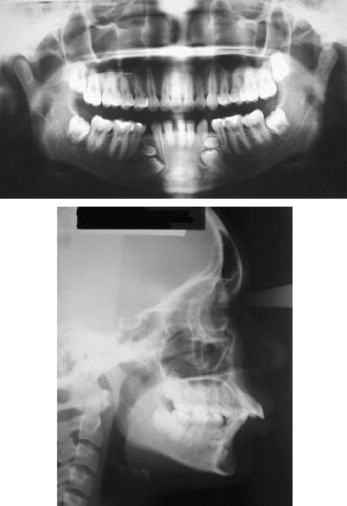
The panoramic radiograph confirmed the presence of the 2 supernumeraries above the mandibular first premolars. The cephalometric analysis showed a skeletal Class II anteroposterior discrepancy with mandibular retrusion. The facial pattern had a slight vertical tendency. Both maxillary and mandibular incisors were tipped labially ( Fig 3 ). The lateral cephalometric radiograph showed the impacted teeth in the mandible.
Treatment objectives
The primary objectives in treating this malocclusion were to eliminate the mandibular spacing and correct the maxillary dentoalveolar protrusion. Additional objectives were to maintain upper lip support for satisfactory facial harmony and the Class I molar relationship. Ideal overjet and overbite relationships were also desirable to improve the esthetics of the occlusion and establish immediate anterior guidance.
Treatment objectives
The primary objectives in treating this malocclusion were to eliminate the mandibular spacing and correct the maxillary dentoalveolar protrusion. Additional objectives were to maintain upper lip support for satisfactory facial harmony and the Class I molar relationship. Ideal overjet and overbite relationships were also desirable to improve the esthetics of the occlusion and establish immediate anterior guidance.
Treatment alternatives
It was obvious that both supernumeraries should be extracted because they were blocking the eruption of the first premolars, and their positions and shapes were unfavorable. Therefore, the main issues were the severity of the mandibular premolar impaction, the arch-length discrepancy and maxillary tooth-size excess, the lack of space for the mandibular premolars, and the proclination of the mandibular and maxillary incisors.
According to these factors, 2 treatment options were presented to the patient. The first included the orthodontic eruption of the mandibular left premolar, after extraction of the supernumerary teeth and the right mandibular premolar. In this situation, the maxillary first premolars would be extracted to maintain a Class I molar relationship and reduce the maxillary incisor proclination. This option would involve placing the mandibular left canine in the position of the left lateral incisor, and the mandibular left first premolar would substitute as a canine. The main advantage of this treatment would be to eliminate the arch-length discrepancy, leaving only a small Bolton tooth-size discrepancy because of the greater mesiodistal canine width.
The second alternative involved extraction of the supernumeraries and the 4 first premolars to maintain a Class I molar relationship, achieve a Class I canine relationship, and reduce the incisor proclination. This treatment option would require anterosuperior stripping to reduce the arch-length discrepancy created by the missing mandibular incisor. This could be achieved by removing approximately 5 mm of interproximal enamel on the maxillary anterior teeth.
Treatment plan
Considering the position of the impacted premolars, the negative space discrepancy, and the patient’s profile, we discussed the treatment options with the patient and her parents. We decided to reposition the mandibular left first premolar. A setup was made to simulate the eventual treatment outcome to ensure that the orthodontic treatment would produce successful results.
Treatment progress
The supernumeraries, the maxillary first premolars, and the mandibular right first premolar were extracted initially. Then surgical access and bonding of the mandibular left premolar were accomplished. Treatment began with banding of the maxillary first molars and placing cervical headgear (GAC International, Central Islip, NY), with 450 g of force. This appliance was to be worn 12 hours a day during leveling and alignment and 16 hours a day during tooth retraction to maintain the Class I molar relationship and allow improvement of the excessive overjet and the incisor proclination.
Fixed 0.022 × 0.028-in preadjusted appliances were placed, and continuous 0.016-in nickel-titanium archwires were placed, with an open-coil spring to obtain space for the mandibular left premolar. When there was enough space, premolar traction was started. Initial alignment was obtained, and the deep bite was corrected with an accentuated reverse curve of Spee. Continuous 0.018 × 0.025-in nickel-titanium archwires were placed to continue leveling and alignment, and elastic chains were used to encourage the premolar to erupt. However, the premolar did not respond to traction, possibly because of tooth ankylosis after the surgical procedure, or perhaps related to the patient’s other tooth anomalies.
After 8 months of unsuccessful treatment, it was decided to extract the remaining mandibular first premolar. To obtain optimal overjet and immediate lateral and anterior guidance, careful stripping of the mesiodistal surfaces of the maxillary anterior teeth was planned. A wax setup was constructed to simulate the treatment effects and avoid increasing the risk of caries and tooth sensitivity.
Continuous 0.019 × 0.025-in stainless steel archwires were then placed, to prepare the teeth for the anterior retraction phase. The maxillary anterior teeth were retracted with maximum anchorage, but no anchorage was used in the mandibular arch. After closure of the extraction spaces, interproximal stripping of the anterior teeth was performed, and the open spaces were consecutively closed by using Class II elastics and 0.020-in and 0.019 × 0.025-in stainless steel archwires in the maxillary and mandibular arches, respectively. Vertical intermaxillary elastics (0.75 in, 2 oz) were used for about 6 weeks to obtain satisfactory tooth interdigitation. The appliances were removed, and a maxillary Hawley retainer and a mandibular fixed retainer were placed for retention. The Hawley retainer was worn full time for 18 months, followed by 6 months of nighttime wear, whereas the lingual retainer would be maintained permanently to enhance the long-term stability of the results. The total treatment time was 34 months.
Treatment results
The patient’s facial esthetics were improved significantly by establishing a passive lip seal ( Fig 4 ). The teeth were well aligned and leveled over the basal bone. Class I molar and canine relationships were established, with ideal overjet and overbite ( Figs 4 and 5 ) . The maxillary dental midline was coincident with the facial midline and with the center of the remaining mandibular central incisor. A mutually protected occlusion was achieved in centric relation, with group function in lateral excursion and anterior guidance in posterior disclusion. Excellent root parallelism was achieved, and root resorption was minimal ( Fig 6 ). Facial esthetics and balance were improved by correcting the maxillary incisor proclination ( Figs 7-9 ). There was improvement of the maxillomandibular relationship (ANB angle and Wits appraisal), incisor inclination, and soft-tissue profile (H and S esthetic lines; naso- and mentolabial angles).


