CHAPTER 3 Second molar extractions
Introduction
The aims of second molar extraction treatment are:
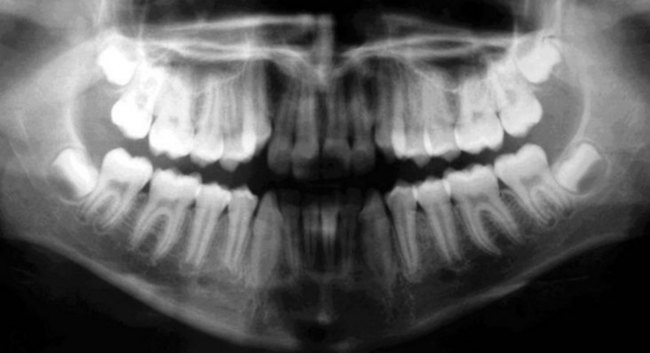
It is important to emphasize that second molar extractions are not a routine procedure in orthodontics and thus frequently are a cause for uncertainty for the majority of clinicians. This is due to, among other concerns, a lack of controlled studies justifying this approach. The majority of publications on second molars extractions are in fact clinical case reports describing the experience of the report’s author(s). However, this approach is a valid treatment option for Class II and Class III malocclusions with the requirements as listed above. The extractions should be done when the third molar tooth germ is forming, with evidence of a well-defined crown of appropriate shape and size1 (Fig. 3.1).

Upper and lower third molars show significant shape variation, such as small or poorly shaped crowns, and are missing in a considerable number of patients. Thus, second molar extractions require careful selection of cases with good-quality third molars, as these teeth will take the place of the extracted second molars (see also next section). According to Richardson and Richardson2 careful selection of the cases guarantees that third molars will erupt in a good or satisfactory position in 90% of the cases, without the need for additional orthodontic realignment.
Development of the second and third molars
The upper second molar is the seventh tooth in each quadrant of the upper and lower dental arches, and is similar to the first molar morphologically, although smaller in size. When describing this tooth, a direct comparison should be made with the first molars, regarding its function and development. In 1935, Schwartz3 evaluated the size of the second molar crown and found the height of the crown varied from 5.7 mm to 8.3 mm. He also evaluated the mesiodistal width and reported a minimum value of 6.5 mm and a maximum value of 10.5 mm.
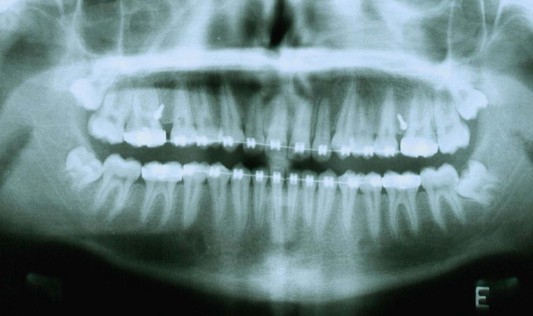
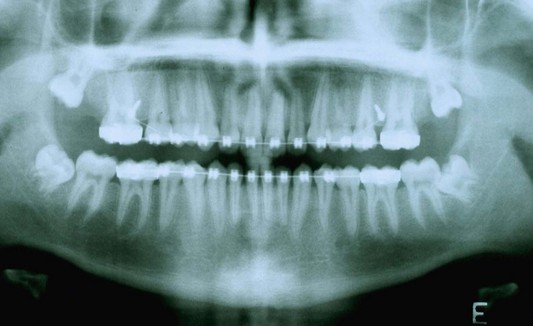
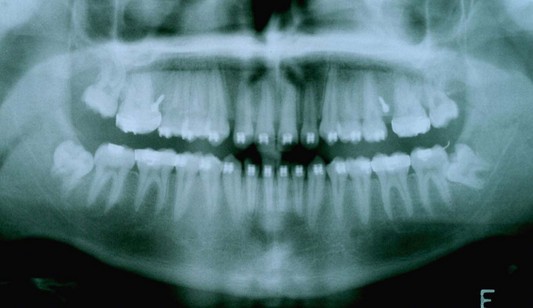
The second molar is also the seventh tooth to erupt, and this normally occurs after the eruption of the second premolars, when a person is 11–13 years of age, depending on their gender. However, the lower second molars usually erupt before the upper ones, within a period of a few months to half a year (Figs 3.2, 3.3 & 3.4). Another important point to consider is the space available to accommodate the second molar.



The upper third molars are considered to be the most variable teeth in the dental arch. Their average mesiodistal width varies from 6.5 mm to 11.5 mm. In 1976, Della Serra4 reported that the upper third molar crowns presented with different shapes, varying from the typical molar shape to much more conical and simpler shapes. To reiterate, this tooth is frequently smaller in size, with a more simple shape. Third molar crowns are also frequently buccally oriented and distally angulated. Due to their anatomical and positional variability, it is critical to carefully select cases that will undergo second molar extraction. The shape and the size of third molars is decisive for the success of treatment.
At the beginning of their formation, upper third molar crowns are angulated distally (Fig. 3.5). However, this tendency decreases as the maxillary tuberosity grows. If there is no growth, third molar impaction is highly likely. If first and second molars are distalized while the third molar is developing, tooth impaction may occur due to the decrease in space in the posterior segment of the dental arch.
Lower third molar eruption is unpredictable, and even if space is available, their satisfactory eruption is not guaranteed. Third molar impaction occurs not only due to a lack of space in the posterior segment of the dental arch, but also due to unfavorable tooth inclination. The best method of avoiding third molar impaction is extraction of the second molars. Such extractions are therefore indicated when the third molar roots are developing (Fig. 3.6).

Why should second molars be extracted?
A large proportion of the routine work of an orthodontist is treating sagittal Class II malocclusions, which is the most common malocclusion among patients seeking orthodontic treatment. Class II malocclusions are frequently accompanied by compromised facial esthetics, which is best dealt with in the mixed dentition. However, patients do not always seek treatment in the mixed dentition. Rather, they postpone treatment to adolescence, a period which is often associated with poor patient cooperation. In such adolescent cases, second molar extractions offers a valid alternative treatment option for Class II treatment.1
As mentioned in the introduction, the main goals of a second molar extraction treatment are preventing third molar impaction (Fig. 3.7) and making first molar uprighting easier. These extractions create some space distal to the archwire, isolating the third molar from the remaining teeth, enabling its anterocclusal movement and its eruption in contact with the distalized first molar (Figs 3.8, 3.9, 3.10, 3.11 & 3.12). A third molar of good shape and size is an ideal substitute for second molars.

Fig. 3.7 Panoramic radiograph showing inadequate space for the eruption of the second and the third molars.


When second molars are extracted, treatment is generally finished with 28 teeth in situ. Therefore, again in a patient with premolar and molar crowding, second molar extraction is a good treatment option. Such a procedure establishes enough space for correction of crowding (Figs 3.13, 3.14, 3.15, 3.16 & 3.17) and avoids third molar impaction.





However, it is to be remembered that second molar extractions cannot replace premolar extractions. The indications for each are entirely different. In summary:4,5
When should second molars be extracted?
Before extracting a second molar, it is necessary to evaluate the shape and the mesiodistal height of its crown, as well as the state of development of the third molar tooth germ. A panoramic radiograph should be taken to check the posterior segments of the dental arches, as it allows satisfactory assessment of third molar size, the amount of root calcification and the relationship between the tooth germ and the second molar root.6 If the radiograph image is blurred, and it is difficult to visualize the size of the third molar germ, it is necessary to take a periapical radiograph. The shape of the third molar is decisive for the treatment plan.
As mentioned briefly in the introduction, the best time to extract second molars is when the crown of the third molar is completely formed and the roots have achieved one-third of their development.7 Thus, the tooth germ of the third molar will move anteriorly, erupting in the space of the second molar and in contact with the distalized first molar (see Fig. 3.1). In over 90% of the cases, third molars erupt in a good or in an acceptable condition after the extraction of the second molars.7 Some upper third molars may erupt in crossbite, and should this occur, it will be necessary to use an orthodontic appliance to correct the bite.
When second molar extraction is carried out in a patient with late maturation of the third molars, the treatment is finished before the third molars erupt. The teeth may take 2 years to erupt after the treatment. Therefore the appliance removal protocol should be to remove the appliance in the lower arch, but keeping the tubes on the molars. This protocol is followed to prevent the extrusion of the lower second molars, which have no antagonist teeth during that period of time (Figs 3.18 & 3.19).


Characteristics of patients who undergo second molar extractions
Graber8 reported that upper second molar extractions would speed up the treatment of Angle Class II division 1 malocclusions. He also described some characteristics that should be observed before submitting a patient to second molar extractions:
Currently, orthodontic treatment is customized according to the facial characteristics of the patient, including certain aspects of the muscle pattern. Second molar extractions are best indicated in patients with mild meso- and dolichofacial patterns, who are the great majority of patients undergoing dental extractions.9 Patients with a horizontal growth pattern and deep overbite are not suitable for second molar extractions, as the dentoalveolar effect of the mechanics applied will result in a clockwise rotation of the occlusal plane,10 thus increasing the already deep overbite. In these cases, some clinical maneuvers are needed to avoid these undesired effects, such as adding reverse curve to the lower archwire.
In summary, the following characteristics of patients are suitable for second molar extractions:
Management of the distalizing mechanics
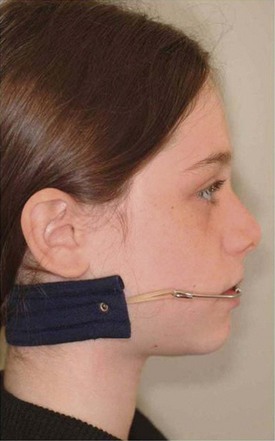
Andrews,11 when developing the Straight-Wire appliance, noted among his findings the mesial angulation of tooth crowns. The whole dentition undergoes anteroposterior movement, caused by the action of the masticatory muscles, that is, the mesial movement of teeth is physiological. Hence when distalization is indicated, the movement in the distal direction is anti-physiologic and difficult to achieve. The recommendation to extract the second or the third molars to create space in the posterior segment of the dental arches and to facilitate easier distalization of the first molars was discussed above.12 The treatment mechanics are customized for each patient and the distalizing device used depends on the facial pattern as well as on the orthodontist’s preference. There are a great variety of devices on the market that can be used to distalize the upper first molars, such as headgear, Class II elastics with sliding jigs and orthodontic miniscrews (Figs 3.20, 3.21 & 3.22).


Eruption of third molars after second molar extraction
As shown by clinical experience, third molars erupt satisfactorily in the vast majority of second molar extraction cases. When second molar extractions are carried out before the formation of the roots of the third molars, the eruption of these teeth is accelerated and frequently occurs by the end of the orthodontic treatment, when the fixed appliances are still in place. If the second molars are extracted when the third molars are late in maturing, the appliances should be removed when the remaining treatment goals have been achieved, even if the third molars are yet to erupt (Figs 3.23 & 3.24, 3.25, 3.26, 3.27, 3.28).






Although, as mentioned already, upper third molars erupt in good or acceptable condition in over 90% of second molar extraction cases, some may erupt in a crossbite. If this occurs, it is necessary to place tubes on the molars to correct the crossbite.2,13
Cavanaugh14 carried out clinical and radiographic evaluation of eruption of the third molars after the extraction of the second molars in 25 subjects. He reported no impactions of the third molars, very low incidence of fused roots and an improvement in the mesiodistal angulation of the third molar roots. He concluded that these extractions, when carried out in carefully selected patients, are the best treatment option in many situations, as it is a reliable and conservative procedure.
In 2007, Zanelato15 studied on study models the position of third molars that had erupted spontaneously in cases treated with second molar extraction and compared this with the position of the third molars in a sample of subjects presenting with normal natural occlusions. The author reported that the third molars, when substituting for the second molars, show good mesiodistal and buccolingual root positions. The size of the clinical crowns of the third molars were acceptable in both the male and the female subjects. No significant difference in clinical crown height was observed between the groups.
1 Zanelato RC, Trevisi HJ, Zanelato A C T. Extração dos segundos molares superiores: uma nova abordagem para tratamentos da Classe I I, em pacientes adolescentes. Revista Dental Press de Ortodontia e Ortopedia Facial. 2000;5:64-75.
2 Richardson ME, Richardson A. Lower third molar development subsequent to second molar extraction. American Journal of Orthodontics and Dentofacial Orthopedics. 1993;104:566-574.
3 Schwartz JR. Practical dental: anatomy and tooth carving. New York: Dental Items of Interest, Henry Kimpton’s Medical Publishing House; 1935.
4 Della Serra O. Anatomia dental, 2nd ed. São Paulo: Artes Mé/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


