CHAPTER 16 Support for the Distal Extension Denture Base
An impression (and resultant stone cast) records the anatomic form of the teeth and their surrounding structures and is needed to make a tooth-supported removable partial denture. The impression should also record the moving tissues that will border the denture in an unstrained position, so the relationship of the denture base to those tissues may be as accurate as possible. Although underextension of the denture base in a tooth-supported prosthesis is the lesser of two evils, an underextended base may lead to food entrapment and inadequate facial contours, particularly on the buccal and labial sides. To accurately record the moving tissues of the floor of the mouth, an individual impression tray should be used, rather than an ill-fitting or overextended stock tray. This has been discussed at length in Chapters 5 and 15.
Factors Influencing the Support of A Distal Extension Base
Contour and Quality of the Residual Ridge
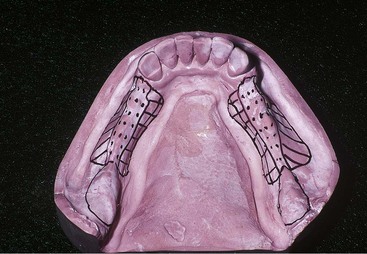
The crest of the bony mandibular residual ridge is most often cancellous. Because lining mucosa restricts both the buccal and lingual mucosae adjacent to teeth in the mandible, loss of firm mucosa overlying the residual ridge is common following tooth extraction in the posterior mandible. Pressures placed on tissues overlying the crest of the mandibular residual ridge usually result in irritation of these tissues, accompanied by the sequelae of chronic inflammation. Therefore the crest of the mandibular residual ridge cannot be a primary stress-bearing region. The buccal shelf region (bounded by the external oblique line and the crest of the alveolar ridge) seems to be better suited for a primary stress-bearing role because it is covered by relatively firm, dense, fibrous connective tissue supported by cortical bone. In most instances this region bears more of a horizontal relationship to vertical forces than do other regions of the residual ridge (Figure 16-1). The slopes of the residual ridge then would become the primary stress-bearing region for resistance of horizontal and off-vertical forces.
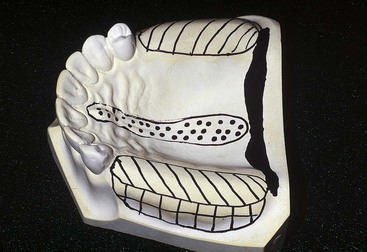
The immediate crest of the bone of the maxillary residual ridge may consist primarily of cancellous bone. Unlike in the mandible, oral tissues that overlie the maxillary residual alveolar bone are usually of a firm, dense nature (similar to the mucosa of the hard palate) or can be surgically prepared to support a denture base. The topography of a partially edentulous maxillary arch imposes a restriction on selection of a primary stress-bearing area. In spite of impression procedures, the crestal area of the residual ridge will become the primary stress-bearing area for vertically directed forces. Some resistance to these forces may be obtained by the immediate buccal and lingual slopes of the ridge. Palatal tissues between the medial palatal raphe and the lingual slope of the posterior edentulous ridge are readily displaceable and cannot be considered as primary stress-bearing sites (Figure 16-2). The tissues covering the crest of the maxillary residual ridge must be less displaceable than the tissues that cover palatal areas, or relief of palatal tissues must be provided in the denture bases or for palatal major connectors.
Extent of Residual Ridge Coverage by the Denture Base
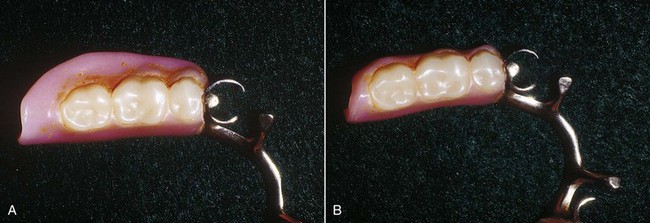
The broader the residual ridge coverage, the greater is the distribution of the load, which results in less load per unit area (Figure 16-3). A denture base should cover as much of the residual ridge as possible and should be extended the maximum amount within the physiologic tolerance of the limiting border structures or tissues. Knowledge of these border tissues and the structures that influence their movement is paramount to the development of broad coverage denture bases. In a series of experiments, Kaires has shown that “maximum coverage of denture-bearing areas with large, wide denture bases is of the utmost importance in withstanding both vertical and horizontal stresses.”
Type and Accuracy of the Impression Registration
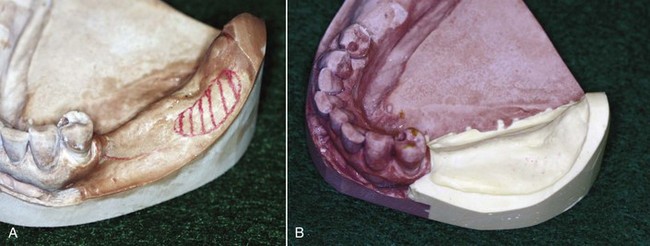
The residual ridge may be said to have two forms: the anatomic form and the functional form (Figure 16-4). The anatomic form is the surface contour of the ridge when it is not supporting an occlusal load. The functional form of the residual ridge is the surface contour of the ridge when it is supporting a functional load.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


