Fig. 6.1
CBCT coronal (a), right and left sagittal (b, d) and axial (c) sections showing massive osteolysis of maxillary sinus floor in the molar region (thin arrow). Right and left maxillary sinuses were partially opacified
Case No. 2
-
50-year-old male.
-
Clinical notes:
-
Difficulty in breathing,
-
Headache,
-
Nasal congestion,
-
Frequent sinusitis (Figs. 6.2 and 6.3).
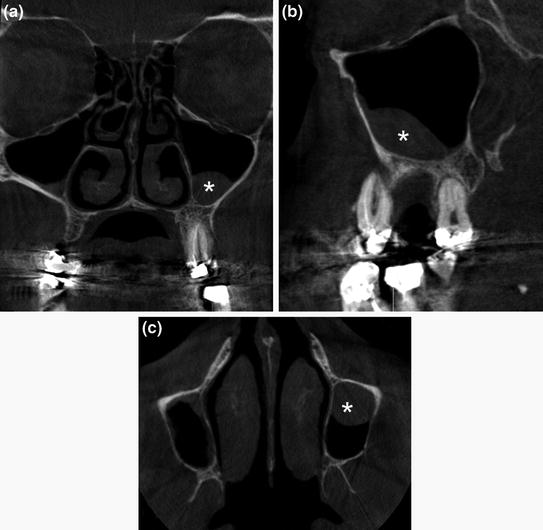 Fig. 6.2CBCT coronal (a), sagittal (b) and axial (c) sections demonstrating mucosal thickening (*) specially in the right maxillary sinus. Note the right and left draining channels (ostium) are opened
Fig. 6.2CBCT coronal (a), sagittal (b) and axial (c) sections demonstrating mucosal thickening (*) specially in the right maxillary sinus. Note the right and left draining channels (ostium) are opened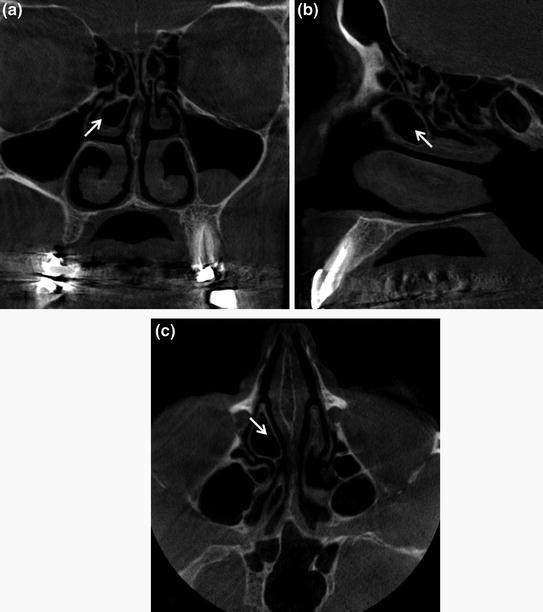 Fig. 6.3CBCT coronal (a), sagittal (b) and axial (c) sections showing the pneumatisation of the right middle turbinate also known as concha bullosa (thin arrow) which can potentially narrow the middle meatus. Note that there is preservation of the air channel between the concha and the nasal septum. Severe deviation of the nasal septum with double curve can be seen
Fig. 6.3CBCT coronal (a), sagittal (b) and axial (c) sections showing the pneumatisation of the right middle turbinate also known as concha bullosa (thin arrow) which can potentially narrow the middle meatus. Note that there is preservation of the air channel between the concha and the nasal septum. Severe deviation of the nasal septum with double curve can be seen
-
Case No. 3
-
66-year-old female.
-
Clinical notes:
-
Headache
-
Chronic upper respiratory tract inflammation for 5 years
-
Therapy with antibiotics and mucolytics, but the problem persists (Fig. 6.4).
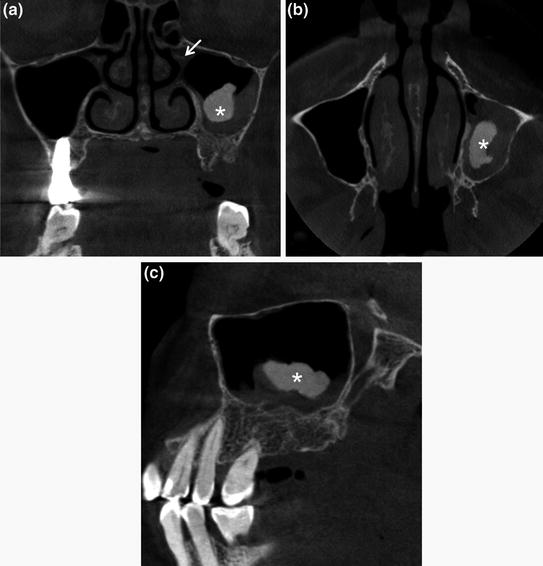 Fig. 6.4CBCT coronal (a) axial (b) and sagittal (c) sections showing irregular calcification tissue (*) at the center of the opacified left maxillary sinus. Note that the omolateral draining channels (ostium) is not preserved (thin arrow)
Fig. 6.4CBCT coronal (a) axial (b) and sagittal (c) sections showing irregular calcification tissue (*) at the center of the opacified left maxillary sinus. Note that the omolateral draining channels (ostium) is not preserved (thin arrow)
-
Case No. 4
-
43-year-old male.
-
Clinical notes:
-
Nasal congestion
-
Headache
-
Facial tenderness, pressure, and pain (Fig. 6.5).
 Fig. 6.5CBCT coronal (a), sagittal (b), and axial (c) sections demonstrating extensive soft tissue inflammation in the right maxillary sinus that appears like an antral mucosal pseudocyst, also called mucoceles (*) and a thin mucosal thickening on the floor of left maxillary sinus. Also note that the nasal septum is deviated with convexity to the right
Fig. 6.5CBCT coronal (a), sagittal (b), and axial (c) sections demonstrating extensive soft tissue inflammation in the right maxillary sinus that appears like an antral mucosal pseudocyst, also called mucoceles (*) and a thin mucosal thickening on the floor of left maxillary sinus. Also note that the nasal septum is deviated with convexity to the right
-
Case No. 5
-
32-year-old male.
-
Clinical notes:
-
In anamnesis allergy and bronchial asthma
-
Headache
-
Nagging pain of the teeth in the left maxilla (Fig. 6.6).
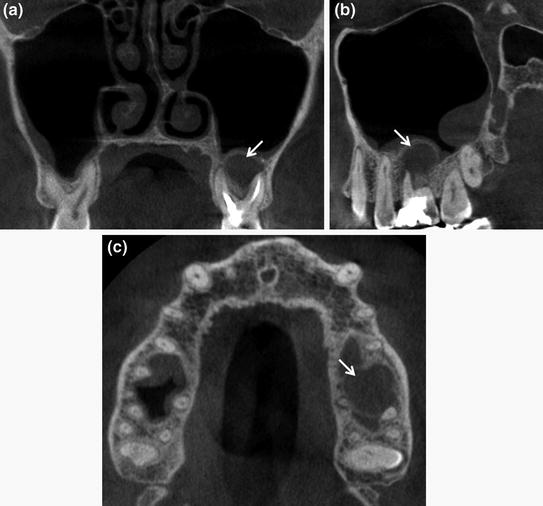 Fig. 6.6CBCT coronal (a), sagittal (b) and axial (c) scans demonstrating presence of odontogenic sinusitis in left paranasal sinus (thin arrow). Note the reactive bone formation within the sinus and the associated mucosal thickening
Fig. 6.6CBCT coronal (a), sagittal (b) and axial (c) scans demonstrating presence of odontogenic sinusitis in left paranasal sinus (thin arrow). Note the reactive bone formation within the sinus and the associated mucosal thickening
-
6.2 Inflammatory Diseases
Case No. 6
-
34-year-old male.
-
Clinical notes:
-
Asymptomatic patient
-
-
Radiopaque lesion found during a routine orthopantomography (Figs. 6.7 and 6.8).
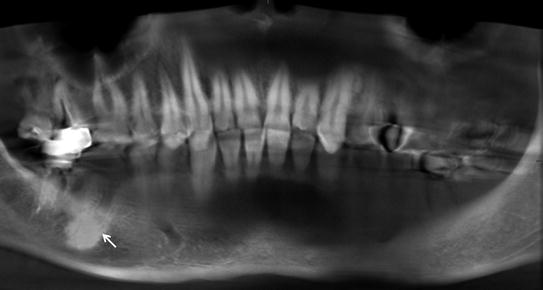 Fig. 6.7CBCT panorex showing bone radiopacity in correspondence of 46 extracted (thin arrow). It seems a periapical inflammatory disease like condensant osteitis
Fig. 6.7CBCT panorex showing bone radiopacity in correspondence of 46 extracted (thin arrow). It seems a periapical inflammatory disease like condensant osteitis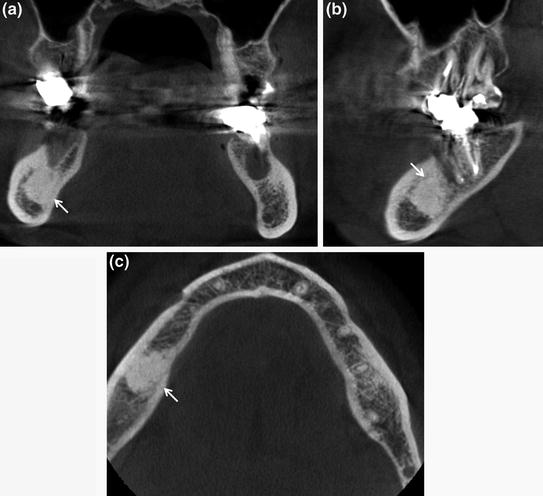 Fig. 6.8CBCT coronal (a), sagittal (b) and axial (c) scans demonstrating, in the right posterior mandible, at the site of 46 extracted, a bone sclerosis that confirms the diagnosis of condensant osteitis (thin arrow)
Fig. 6.8CBCT coronal (a), sagittal (b) and axial (c) scans demonstrating, in the right posterior mandible, at the site of 46 extracted, a bone sclerosis that confirms the diagnosis of condensant osteitis (thin arrow)
Case No. 7
-
42-year-old male.
-
Clinical notes:
-
Persistent pain in 16–17 area, even after root canal therapy (Figs. 6.9 and 6.10).
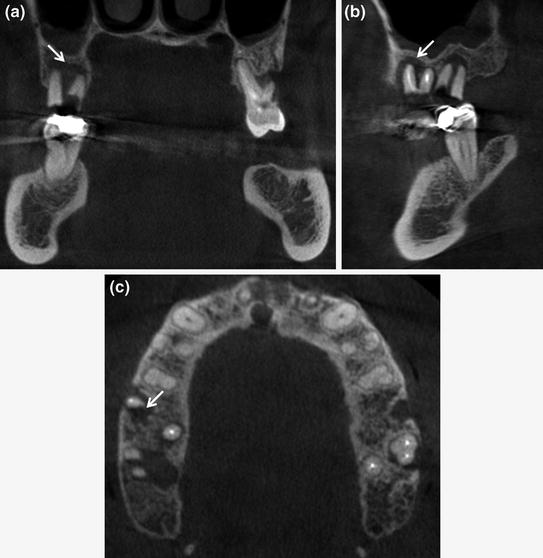 Fig. 6.9CBCT coronal (a), sagittal (b) and axial (c) sections showing a wide radiolucent periradicular area dependent to the element 16 surrounding the mesial root (thin arrow). The radiographic signs suggest periradicular periodontitis
Fig. 6.9CBCT coronal (a), sagittal (b) and axial (c) sections showing a wide radiolucent periradicular area dependent to the element 16 surrounding the mesial root (thin arrow). The radiographic signs suggest periradicular periodontitis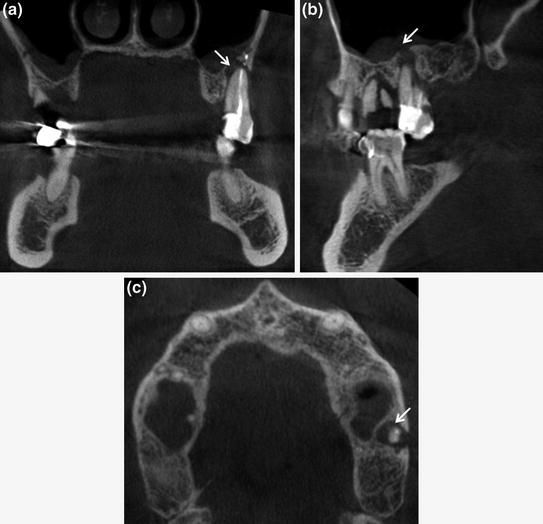 Fig. 6.10CBCT coronal (a), sagittal (b) and axial (c) sections demonstrating the presence of an extensive periradicular lesion associated with tooth 27 (thin arrow). Note the degree of root resorption that determinate a periapical osteolysis
Fig. 6.10CBCT coronal (a), sagittal (b) and axial (c) sections demonstrating the presence of an extensive periradicular lesion associated with tooth 27 (thin arrow). Note the degree of root resorption that determinate a periapical osteolysis
-
Case No. 8
-
58-year-old male.
-
Clinical notes:
-
Pain after root canal therapy of 45
-
Large spectrum antibiotic therapy (Fig. 6.11).
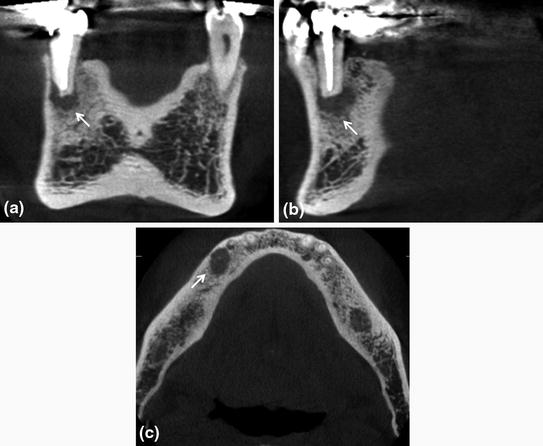 Fig. 6.11CBCT coronal (a), sagittal (b) and axial (c) sections evidencing an area of low density at the apex of 45 tooth (thin arrow). It is a chronic periapical osteoperiostitis, or “halo lesion” determining displacement of the periosteum
Fig. 6.11CBCT coronal (a), sagittal (b) and axial (c) sections evidencing an area of low density at the apex of 45 tooth (thin arrow). It is a chronic periapical osteoperiostitis, or “halo lesion” determining displacement of the periosteum
-
Case No. 9
-
24-year-old male.
-
Clinical notes:
-
Pain on the I quadrant, in 16–17 area, worsening with hot food and/or drinks and lying
-
Sometimes right eye swollen (Figs. 6.12 and 6.13).
 Fig. 6.12CBCT panorex: well-defined, corticated, wide ovoid radiopaque area extending from 16 to 17 tooth (*). Note the conservative restoration of 25, 36 and 46
Fig. 6.12CBCT panorex: well-defined, corticated, wide ovoid radiopaque area extending from 16 to 17 tooth (*). Note the conservative restoration of 25, 36 and 46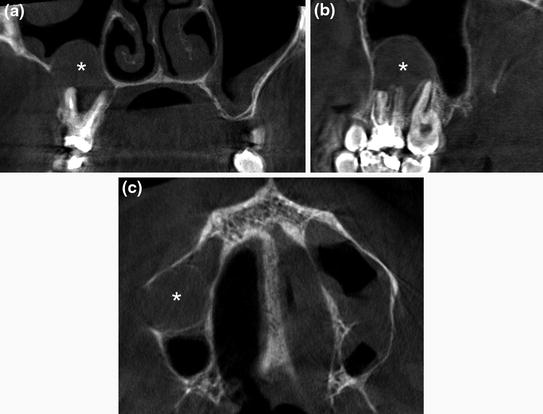 Fig. 6.13CBCT coronal (a), sagittal (b) and axial (c) sections showing an oval radiopaque with well-defined peripheral borders (*). The pathology involves the apical region of tooth 16 and 17, and protrudes into the adjacent right maxillary sinus. Note the moderate bilateral maxillary sinus mucosal thickening without blockage of both osteomeatal complexes
Fig. 6.13CBCT coronal (a), sagittal (b) and axial (c) sections showing an oval radiopaque with well-defined peripheral borders (*). The pathology involves the apical region of tooth 16 and 17, and protrudes into the adjacent right maxillary sinus. Note the moderate bilateral maxillary sinus mucosal thickening without blockage of both osteomeatal complexes
-
Case No. 10
-
47-year-old female.
-
Clinical notes:
-
Pain on III quadrant mostly during mastication
-
Feeling a bad taste in the mouth
-
Swallowing pus and blood
-
High bleeding index at the periodontal probing and washing her teeth (Fig. 6.14).
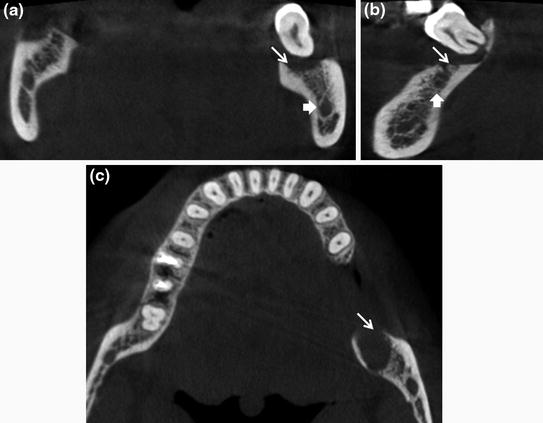 Fig. 6.14CBCT coronal (a), sagittal (b) and axial (c) sections showing a radiolucent area in close proximity to teeth 38 (thin arrow). The mandibular canal (arrow) is not involved
Fig. 6.14CBCT coronal (a), sagittal (b) and axial (c) sections showing a radiolucent area in close proximity to teeth 38 (thin arrow). The mandibular canal (arrow) is not involved
-
6.3 Benign Neoplastic Lesions
Case No. 11
-
41-year-old female.
-
Asymptomatic lesion found during a routine orthopantomography (Fig. 6.15).
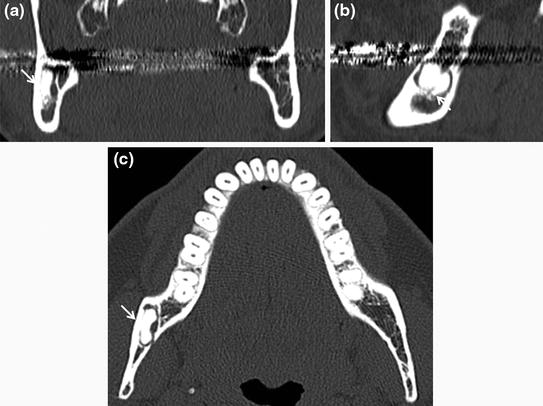 Fig. 6.15CBCT coronal (a), sagittal (b) and axial (c) sections showing well-defined radiopaque lesion (thin arrow) in the posterior branch of the mandible. The lesion is surrounded by radiolucent band and radiopaque cortex giving it a target appearance. There are no signs of root resorption and of invasion of mandibular canal. The radiographic signs suggest a benign process and are consistent with complex odontoma
Fig. 6.15CBCT coronal (a), sagittal (b) and axial (c) sections showing well-defined radiopaque lesion (thin arrow) in the posterior branch of the mandible. The lesion is surrounded by radiolucent band and radiopaque cortex giving it a target appearance. There are no signs of root resorption and of invasion of mandibular canal. The radiographic signs suggest a benign process and are consistent with complex odontoma
Case No. 12
-
11-year-old male.
-
Asymptomatic lesion found during a routine orthopantomography to evaluate the dental growth (Fig. 6.16).
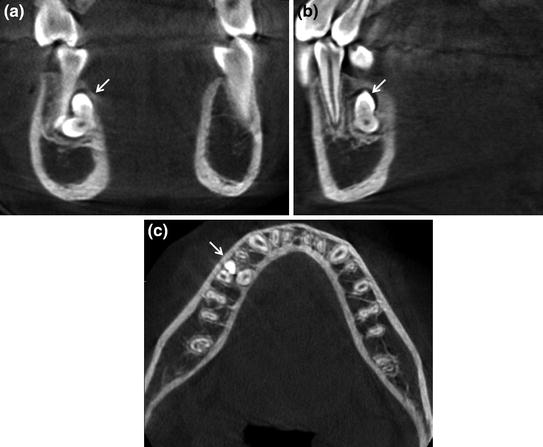 Fig. 6.16CBCT coronal (a), sagittal (b) and axial (c) sections demonstrating, in correspondence of the lingual plate of the root of 45, a radiopaque masse that has tooth like appearance and density (thin arrow). The radiographic signs suggest a benign process and are consistent with compound odontoma
Fig. 6.16CBCT coronal (a), sagittal (b) and axial (c) sections demonstrating, in correspondence of the lingual plate of the root of 45, a radiopaque masse that has tooth like appearance and density (thin arrow). The radiographic signs suggest a benign process and are consistent with compound odontoma
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


