A 12-year-old girl presented with a Class II Division 1 malocclusion, complicated by a complete transposition of the maxillary left canine into the position normally occupied by the left lateral incisor. Dental and medical histories were noncontributory. Brackets were bonded on all maxillary teeth, from first molar to first molar, except for the left lateral incisor. Because the lateral incisor was not engaged on the archwire, the tooth was free to physiologically move out of the path of canine root movement. To prepare the site for canine retraction, a coil spring was used to open space between the left central incisor and the first premolar. A 2 × 12-mm stainless steel miniscrew was placed in the infrazygomatic crest, labial to the mesiodistal cusp of the maxillary left first molar. A 0.019 × 0.025-in titanium-molybdenum alloy T-loop, anchored by the miniscrew, was used to retract the canine root over the labial surface of the root of the distally positioned lateral incisor. In 24 months, this difficult malocclusion, with a Discrepancy Index score of 18, was treated to a Cast-Radiograph Evaluation score of 26.
Highlights
- •
Segmented mechanics are optimal for individualized movement of target teeth.
- •
Continuous archwires to correct a transposition invite root resorption.
- •
Skeletal anchorage was used to retract the canine and correct the Class II relationship.
- •
T-loop springs anchored with a bone screw were effective for this patient.
Tooth transposition is defined as a change in position of 2 adjacent teeth in the same quadrant, but the clinical presentation may be quite variable. It is identified as a complete transposition when the crowns and the roots of the involved teeth exchange places in the dental arch, and as an incomplete transposition when the crowns are transposed but the roots remain in their normal positions. The prevalence of transposition is about 0.4%. Tooth transpositions occur more commonly in the maxilla than in the mandible, and the maxillary permanent canine is the most frequently involved tooth.
Tooth transpositions are more commonly observed in female patients and may occur unilaterally or bilaterally. There is a greater frequency of unilateral transpositions on the left side. Transpositions are often associated with peg-shaped or congenitally missing maxillary lateral incisors, retention of deciduous canines, malposed adjacent teeth, and rotations.
Several etiologic factors have been proposed: genetics, interchange in the position of the developing tooth buds, trauma, mechanical interferences, early loss of deciduous teeth, and prolonged retention of deciduous teeth. However, the latter is more often a sequela of transposition rather than an etiologic factor.
Peck et al classified transpositions as follows: (1) maxillary canine-first premolar, (2) maxillary canine-lateral incisor, (3) maxillary canine to first molar site, (4) maxillary lateral incisor-central incisor, (5) maxillary canine to central incisor site, and (6) mandibular lateral incisor-canine.
This patient had a complete transposition of the maxillary left canine and lateral incisor.
Diagnosis and etiology
The clinical examination of this 12-year-old girl in the permanent dentition showed an Angle Class II molar malocclusion with a complete transposition of the maxillary left canine and lateral incisor ( Figs 1 and 2 ). The ectopic eruption of the maxillary left canine positioned it high in the vestibular fold between the central and lateral incisors ( Figs 3 and 4 ).

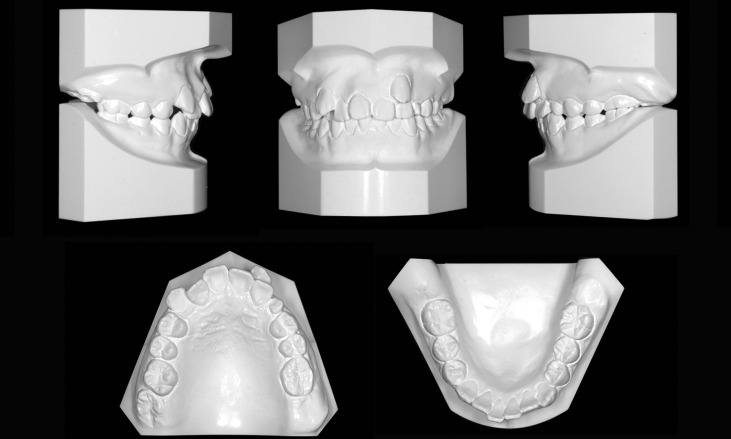


From the patient’s perspective, the anomaly was camouflaged by normal midlines and a functional deciduous canine, so the chief complaint was crowding of the maxillary arch. The asymmetric overjet had a maximum of 5 mm, but the lateral facial profile was acceptable. A mild mandibular tooth size-arch length discrepancy was noted. The intraoral examination showed that the maxillary right second molar was partially erupted, but the other 3 second molars were unerupted.
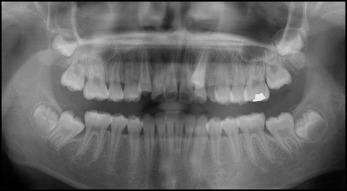
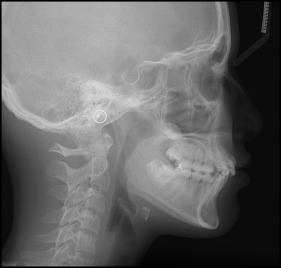
A panoramic radiograph documented that all permanent teeth, including the third molars, were present ( Fig 5 ). The cephalometric analysis was consistent with a Class II skeletal pattern and a mild tooth size arch width discrepancy ( Fig 6 ). There was increased axial inclination of both the maxillary and mandibular incisors. The cephalometric measurements are summarized in the Table .
| Pretreatment | Posttreatment | Difference | |
|---|---|---|---|
| Skeletal analysis | |||
| SNA (°) | 81 | 80 | 1 |
| SNB (°) | 77 | 76 | 1 |
| ANB (°) | 4 | 4 | 0 |
| SN-MP (°) | 36 | 36 | 0 |
| FMA (°) | 24 | 23 | 1 |
| Dental analysis | |||
| U1 to NA (mm) | 5 | 1 | 4 |
| U1 to SN (°) | 113 | 104 | 9 |
| L1 to NB (mm) | 6 | 5 | 1 |
| L1 to MP (°) | 101 | 98 | 3 |
| Facial analysis | |||
| E-line to UL (mm) | −1 | −2 | 1 |
| E-line to LL (mm) | 1 | 0 | 1 |
| E-line to LL (mm) | −0.5 | −2 | 1.5 |
Treatment objectives
The treatment objectives were to (1) establish functional Class I molar and canine relationships, (2) correct the transposition and restore natural tooth order, (3) create ideal overbite and overjet, (4) correct incisor inclinations and root angulations, and (5) improve facial esthetics.
Treatment objectives
The treatment objectives were to (1) establish functional Class I molar and canine relationships, (2) correct the transposition and restore natural tooth order, (3) create ideal overbite and overjet, (4) correct incisor inclinations and root angulations, and (5) improve facial esthetics.
Treatment alternatives
Compared with the mandibular arch, there are more therapeutic options for the maxillary dentition because the supporting bone is less dense. Esthetically and functionally, it is generally preferable to move transposed teeth to their normal positions in the arch.
Consistent with the treatment objectives, the most conservative treatment plan was nonextraction alignment of the malposed teeth. Bilateral infrazygomatic crest (IZC) bone-screw anchorage was indicated to retract the transposed canine and correct the Class II malocclusion. To prevent root interference or resorption during the retraction process, the transposed canine was maintained in a high position as it was retracted to take advantage of the tapered root structure of adjacent teeth.
A second treatment plan was to extract the transposed canine and substitute the first premolar for the canine. Although this approach is less challenging technically, there are multiple compromises in outcomes associated with retaining Class II buccal segments: esthetics, periodontal, and functional.
The third treatment option was to extract the left permanent and deciduous canines and restore the canine with a dental implant. Considering the growth potential of this young patient, an osseointegrated implant was an undesirable choice. After carefully considering all the options, the first treatment plan was selected: correct the canine transposition and the Class II buccal relationship with IZC bone-screw anchorage.
Treatment progress
Treatment was started in the maxillary arch, with a 0.022-in passive self-ligation system (Damon 3mx; Ormco, Glendora, Calif); low-torque brackets were placed on the incisors. An open-coil spring was placed between the left central incisor and the first premolar to create space. One week later, the deciduous canine was extracted, and 2 OrthoBoneScrews (2 × 12 mm) with 0.022 × 0.028-in rectangular openings (Newton’s A, Hsinchu, Taiwan) were inserted bilaterally in the IZCs, buccal to the maxillary first molars. Low-tension (2 oz) power chains were attached from the first premolars to the screws bilaterally ( Fig 7 ).
A T-loop of 0.019 × 0.025-in titanium-molybdenum alloy was inserted in the hole of the left OrthoBoneScrew and activated to retract the left canine. As designed, the T-loop retracted the transposed canine while maintaining its position high in the vestibular fold. After 1 month, a power tube was activated from the left first premolar to the canine. When activated, the T-loop produced a root distal moment on the canine ( Fig 8 ). After 3 months of traction, the transposed canine was translated about 4 mm distally ( Fig 9 ).


