The permanent canine is the most frequently displaced or impacted tooth. The standard treatment for an impacted canine includes surgical exposure and orthodontic alignment. Autotransplantation is a treatment alternative for canines with complete root formation. The purpose of this article is to report a canine autotransplantation where the extraction site was preserved with a titanium prosthesis and a bioresorbable membrane. The autotransplanted canine had minimal root resorption and no ankylosis.
Permanent canines are important both functionally and esthetically. However, they are also the most frequently displaced and impacted teeth in the dentition. The standard method to manage an impacted canine includes surgical exposure and orthodontic alignment, but such treatment is often impractical.
Autotransplantation of teeth with completed root formation is an alternative to orthodontic treatment, and this process refers to the autogenous repositioning of a tooth in a surgically formed socket to replace a tooth that might be congenitally missing or have severe caries.
Autogenous transplantation of impacted canines was tried by Widman in 1915. Root resorption is often found after autotransplantation surgery. The prevalence of external root resorption is high, and it is the most common cause of the eventual failure of the autotransplanted teeth. Periodontal healing is responsible for root resorption after autotransplantation. Periodontal cells located at the surface of the transplanted roots are known to facilitate ankylosis and root resorption. Preparing a suitable recipient site and protecting the periodontal cells from damage should increase the success rate of autotransplantation.
In this case report, we describe extraction site preservation by fixation with a titanium prosthesis and a bioresorbable membrane, and their effects on the autotransplanted canine during and after orthodontic treatment.
Diagnosis and etiology
The patient was a 14-year-old adolescent boy who was referred by his dentist for an orthodontic consultation with the chief complaint of a missing canine. He was healthy with no remarkable medical history and had no contraindication for dental treatment. No signs or symptoms of temporomandibular disorders according to the guidelines of the American Academy of Orofacial Pain were reported.
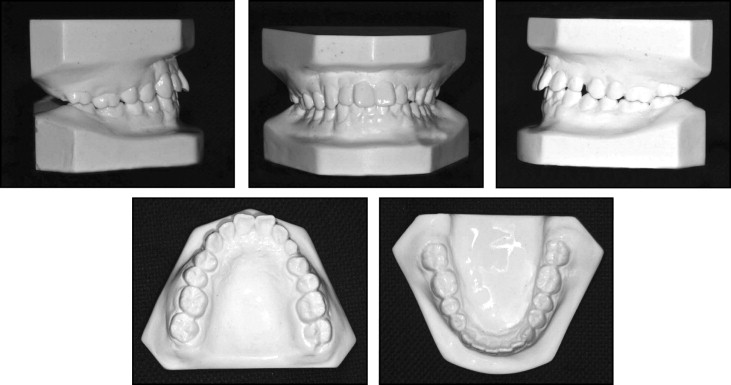
The pretreatment records showed that the patient had normal vertical facial proportions, a straight profile, and good facial symmetry. The pretreatment intraoral photographs showed that the maxillary left deciduous canine was retained and decayed ( Fig 1 ).

Analysis of the dental casts disclosed a Class II molar relationship tendency on the both sides and several mildly rotated teeth. The maxillary overjet was 3.5 mm, and the patient had a normal overbite and no crossbites. The maxillary and mandibular midlines were coincident ( Fig 2 ).
The panoramic radiograph showed that the maxillary left canine was impacted at the apex of the maxillary left lateral incisor, and this incisor had obvious root resorption because of the impacted canine. No radiographic signs of the third molars were visible at the beginning of the treatment ( Fig 3 ).
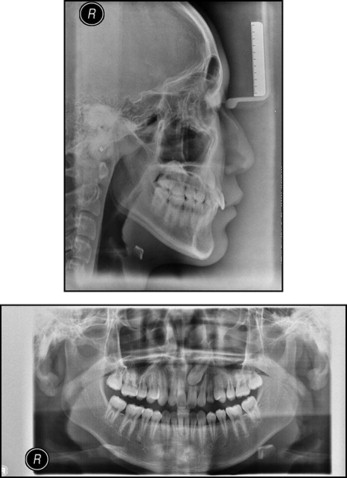
The cephalometric evaluation confirmed a Class I skeletal relationship with an average growth pattern. The maxillary dentition was placed normally on its base, but the mandibular dentition was retracted. The vertical relationships appeared to be within normal limits ( Table ).
| Pretreatment | Posttreatment | Two years posttreatment | |
|---|---|---|---|
| SNA (°) | 83.1 | 84.3 | 85.2 |
| SNB (°) | 81.5 | 83.2 | 84.2 |
| ANB (°) | 1.6 | 1.1 | 1 |
| FMA (°) | 29.3 | 29.4 | 29.7 |
| U1 to NA length (mm) | 2.4 | 7.5 | 7.3 |
| U1 to NA angle (°) | 16.8 | 30.5 | 30 |
| L1 to NB length (mm) | 1.6 | 5.3 | 5.5 |
| L1 to NB angle (°) | 22.7 | 29.1 | 29 |
| Wits (mm) | −1.8 | −3.3 | −3.5 |
Treatment objectives
Autotransplantation of a tooth can obviously shorten the treatment time when a suitable donor tooth is available and the anatomic circumstances permit this procedure. The treatment objectives included extracting the retained deciduous canine, transplanting the impacted canine into the extraction site, and establishing a Class I molar relationship on both sides along with normal overjet and overbite.
Treatment objectives
Autotransplantation of a tooth can obviously shorten the treatment time when a suitable donor tooth is available and the anatomic circumstances permit this procedure. The treatment objectives included extracting the retained deciduous canine, transplanting the impacted canine into the extraction site, and establishing a Class I molar relationship on both sides along with normal overjet and overbite.
Treatment alternatives
One treatment alternative for this patient was to extract the deciduous canine and move the permanent canine into position orthodontically. This option would take 2 to 3 years and could jeopardize the root of the maxillary left lateral incisor.
The second option was to extract both the deciduous canine and the impacted permanent canine, adjust the canine space orthodontically, keep the space until adulthood, and place an implant in the canine space. However, from the esthetic point of view, the patient would not tolerate the missing canine throughout adolescence. Furthermore, after removal of the tooth, the alveolar processes would begin to atrophy, affecting the maintenance of the alveolar bone and the attached gingiva.
The other option was extraction of the left lateral incisor and the deciduous canine with canine transposition into the lateral incisor site orthodontically. After orthodontic treatment, a veneer could be placed on the canine to match the morphology of the contralateral incisor, and a future implant would be placed in the left canine position. However, the success of this treatment option depends on the success of the extrusion of the impacted canine, the future cost of an implant, and the appearance of the incisor’s gingiva.
Treatment progress
After discussion with the oral surgeon, who performed the autotransplant surgery, we decided to treat with full fixed appliances, incorporating extraction of the deciduous canine and autotransplantation of the impacted canine into the extraction site.
Before the orthodontic treatment, we could not accurately identify the position of the impacted tooth on the pretreatment panoramic radiograph. A medical computerized tomography scan was planned to assess the position of the canine relative to the root of the lateral incisor.
The composite image showed complete transposition, with the crown of the canine mesial to the root of the lateral incisor, yet palatal to the root of the incisor ( Fig 4 ). Degeneration of alveolar bone would most likely occur after extraction; thus, to maintain the height of the alveolar ridge, a pure titanium canine prothesis was planned for the extraction site. With the computerized tomography images, 2 acrylic teeth were made, and the sizes were the same as the impacted tooth. One was for the autotransplantion surgery to prepare the recipient site, and the other was invested, cast, and soldered with special equipment in an oxygen-free environment to produce a pure titanium canine prothesis.
Fixed appliances (Mini Uni-Twin, 0.022-in slot; 3M Unitek, Monrovia, Calif) were placed on the maxillary and mandibular teeth in February 2009. A nickel-titanium open-coil spring was used to gain more space for the donor tooth. Within 6 months of leveling and alignment, stainless steel overlay arches (0.019 × 0.025 in) were placed in the maxillary and mandibular arches for stabilization, and the space in the recipient site was prepared for the transplant ( Fig 5 , A ). The recipient site was the same size as the acrylic tooth. At this time, the molar and canine relationships were Class I on the right side, with a Class II tendency on the left side because the impacted canine was smaller than the right canine.
The deciduous canine was extracted, and the extraction site was maintained to implant the titanium canine prosthesis ( Fig 5 , B ). After a month of recovery, the titanium prosthesis was removed, and the extraction site was the same as the titanium prosthesis, with no inflammation. The impacted canine was extracted and transplanted into the extraction site. Because there was not enough bone on the buccal alveolar process, we placed a xenograft of deproteinized bovine bone mineral (Bio-Oss; Geistlich, Wolhusen, Switzerland) between the root and the gingival flap. We also placed a bioresorbable membrane between the bone substitute and the gingival flap ( Fig 6 ). We removed the donor tooth’s occlusal contact for early stability in the first 2 weeks and used a 0.012-in nickel-titanium segment wire to level and align the autotransplanted tooth into its normal position ( Fig 5 , C and D ). One month after the transplantation surgery, root canal treatment was performed ( Fig 7 , B ). During the final stages, Class II elastics and anterior box elastics were used to idealize the occlusion.


