Asymmetries are among the most challenging problems in orthodontics. Proper diagnosis is critical to discern first whether the asymmetry is dental or skeletal. If it is dental, one must then determine whether one dental arch or both are at fault. Once diagnosed, the next challenge is determining not only an appropriate treatment plan, but also the appropriate mechanics plan. This aim of this article is to present a patient with a severe asymmetry to emphasize the importance of a problem-based differential diagnosis to develop both a sound treatment plan and a mechanics plan that successfully integrates miniscrews from the start of the process. An 18-year-old woman had a Class III subdivision left malocclusion, an asymmetric lower facial third, and a deviated midline. The treatment plan consisted of asymmetric distalization of the maxillary right and mandibular left posterior dentitions to create space to resolve the deviated midlines, correct the canted occlusal plane, and obtain an ideal occlusion. Active treatment with Clarity ceramic 0.022 × 0.028-in appliances (3M Unitek, Monrovia, Calif), temporary anchorage devices, and a pendulum appliance lasted 22 months. The final result and the 2-year retention records demonstrate that a harmonious facial balance, an attractive smile, ideal occlusal relationships, and a stable outcome were achieved. This case report shows that with proper planning, asymmetric use of temporary anchorage devices in multiple posterior quadrants can be used to obtain molar distalization, and this approach is an effective alternative to dental extraction therapy.
Highlights
- •
The case shows the asymmetric use of temporary anchorage devices (TADs) in multiple posterior quadrants for molar distalization.
- •
TADs also help to resolve the deviated midlines and correct the canted occlusal plane.
- •
With proper planning, TADs are an effective alternative to dental extraction therapy.
Symmetry is an essential component in the perception of dental esthetics and is one of the most important factors in defining the attractiveness of a smile. Smile esthetics has also been regarded as a requirement for successful treatment by both orthodontists and patients. To achieve this, a common goal of orthodontic treatment is to achieve maxillary and mandibular midlines that are coincident not only with each other, but also with the facial midline. Asymmetric dental midlines and molar relationships can adversely affect facial and smile esthetics and also the functional component of the occlusion.
For asymmetric molar relationships, unilateral distalization is a challenge for orthodontists. Multiple treatment methods and appliances for molar distalization have been described. Molar distalization appliances can be intraoral or extraoral. Extraoral appliances such as headgear are efficient for distalizing molars, but they require patient cooperation and consistent wear. Previous investigations have shown that patient cooperation decreases over time and that determining who will be compliant is unpredictable. Conventional intraoral appliances such as the pendulum, which combines a Nance button with open nickel-titanium springs or beta-titanium alloy cantilevers, can effectively distalize the molars. However, these conventional appliances show that anchorage loss results in mesialization of the anterior anchorage units, including premolar tipping, extrusion, and anterior protrusion, either indirectly or directly.
Temporary anchorage devices in other applications have been shown to optimize orthodontic mechanics, require minimal patient cooperation, and minimize the adverse side effects mentioned above. Recent studies have been directed toward the use of miniscrews and miniplates for intrusion or distalization of the mandibular posterior teeth. A distalizing force is applied through a nickel-titanium coil spring while connecting the miniscrew to hooks on the archwire for indirect anchorage. Because the force to move the anterior teeth forward is resisted, the side effects are minimized, resulting in the desired treatment effect of distal movement of the posterior teeth while maintaining or in some cases simultaneously uprighting the anterior teeth. This case report builds on earlier work to describe asymmetric and unilateral distalization of the posterior dentition to treat a Class III subdivision left malocclusion with a canted occlusal plane and a deviated midline with the successful use of miniscrews.
Diagnosis and etiology
A young Chinese woman, aged 18 years 2 months, came for an orthodontic evaluation at Orthodontic department of Nanjing Stomatological Hospital with chief complaints of an asymmetric lower face and deviated dental midlines upon smiling. The clinical examination demonstrated mandibular anterior dental crowding and a unilateral left anterior crossbite with a functional shift. The patient reported a functional deficit: she could masticate only on her right side for the past 6 years. Her goals included obtaining ideal facial esthetics and an ideal functional occlusion. Her medical history was noncontributory.
The pretreatment facial photographs ( Fig 1 ) show a straight facial profile, normal vertical facial proportions, and an asymmetric lower face especially on smiling. She had a skeletal Class I relationship with dental Class III subdivision left malocclusion (Class I right molar and canine, and Class III left molar but Class I left canine relationships). The maxillary and mandibular arch forms were asymmetric and not coordinated. Other findings included a labially tipped mandibular left canine, mild maxillary arch crowding (3 mm), and moderate mandibular arch crowding (6 mm). She had a deep curve of Spee (4 mm) ( Fig 2 ), and there was minimal occlusal contact of the mandibular left second molar and its opposing tooth because of the Class III molar relationship. The maxillary and mandibular dental midlines were coincident with each other, although both were to the left of the midsagittal plane by 2.5 mm, with the maxillary central incisors tipped to the left and a canted occlusal plane. Oral hygiene was adequate. The patient reported no pain in the temporomandibular joint region; however, an occasional unilateral left click was observed on wide opening with reduced bite force on the left side.


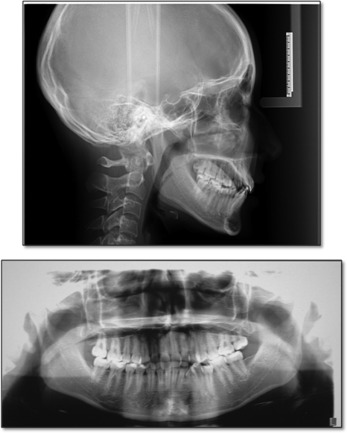
The panoramic radiograph showed a full complement of permanent teeth (except for the third molars), mesially tipped mandibular left molars, and no mandibular skeletal asymmetry ( Fig 3 ). The cephalometric analysis indicated that the maxilla and the mandible were normally positioned to the cranial base (SNA, 83.5°; SNB, 80°). The ANB angle (3.5°) indicated a Class I skeletal relationship. The mandibular plane was normal relative to the cranial base (SN-MP, 31°). The maxillary and mandibular incisors were slightly upright (U1-SN, 99.0°; U1-NA, 20.0°; LI-NB, 22.0°) ( Fig 3 ; Table ). The patient was diagnosed with a skeletal Class I malocclusion, a Class III subdivision left molar relationship, and deviated midlines.
| Measurements | Chinese norm | Pretreatment | Posttreatment | Difference |
|---|---|---|---|---|
| SNA (°) | 82.8 | 83.5 | 83.7 | 0.2 |
| SNB (°) | 80.1 | 80.0 | 80.1 | 0.1 |
| ANB (°) | 2.7 | 3.5 | 3.6 | 0.1 |
| Wits (mm) | −1.15 | −1.05 | −1.00 | 0.05 |
| FH-NP (°) | 85.4 | 88.6 | 88.0 | −0.6 |
| SN-MP (°) | 32.5 | 31.0 | 31.3 | 0.3 |
| FMA (°) | 27.3 | 20.5 | 21.5 | 1.0 |
| U1 to SN (°) | 105.7 | 99.0 | 101.5 | 2.5 |
| U1 to NA (°) | 22.8 | 20.0 | 22.0 | 2.0 |
| U1 to NA (mm) | 5.1 | 3.0 | 3.7 | 0.7 |
| L1 to NB (°) | 30.3 | 22.0 | 24.0 | 2.0 |
| L1 to NB (mm) | 6.7 | 3.0 | 4.0 | 1.0 |
| L1 to MP (°) | 96.9 | 88.0 | 90.0 | 2.0 |
| U1/L1 (°) | 124.2 | 142.0 | 139.0 | −3.0 |
| Upper lip (mm) | −1.4 | −4.0 | −3.5 | 0.5 |
| Lower lip (mm) | 0.6 | −3.0 | −2.3 | 0.7 |
Treatment objectives
Based on the initial records and the patient’s desires to avoid extractions, the treatment objectives were to level and align the dental arches, perform asymmetric distalization of both the maxillary right and the mandibular left posterior quadrants to achieve Class I canine and molar relationships bilaterally, obtain coincident dental and facial midlines, and correct the canted occlusal plane. To accomplish these goals, conventional full fixed appliances, a unilaterally activated pendulum appliance, and asymmetric miniscrews were planned.
Treatment objectives
Based on the initial records and the patient’s desires to avoid extractions, the treatment objectives were to level and align the dental arches, perform asymmetric distalization of both the maxillary right and the mandibular left posterior quadrants to achieve Class I canine and molar relationships bilaterally, obtain coincident dental and facial midlines, and correct the canted occlusal plane. To accomplish these goals, conventional full fixed appliances, a unilaterally activated pendulum appliance, and asymmetric miniscrews were planned.
Treatment alternatives
In many asymmetry cases, particularly dental asymmetries, an asymmetric extraction plan is often considered. For this patient, we thought that the asymmetric dental midline and the unilateral left full cusp Class III molar relationship could not be corrected; the left second molars would have had no opposing teeth. In addition, the patient and her parents did not want dental extractions. Other possible treatment alternatives included asymmetric maxillary molar distalization with an extraoral appliance and mandibular asymmetric distalization with a lip bumper. The patient refused these because of the visibility of the headgear and the perceived discomfort, and the parents requested nonremovable treatment.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


