This case report describes the use of a microimplant-assisted rapid palatal expansion (MARPE) appliance to orthopedically correct a transverse maxillary deficiency in an adult patient. Expansion forces transmitted through the teeth in traditional rapid palatal expansion appliances create unwanted dental effects rather than true skeletal expansion, particularly in older patients with more rigid interdigitation of the midpalatal suture. This 19-year-old patient had maxillary constriction with a unilateral posterior crossbite. A MARPE appliance secured to the palatal bones with 4 microimplants was expanded by 10 mm. Pre-MARPE and post-MARPE cone-beam computed tomography cross sections demonstrated 4 to 6 mm of expansion of the maxillofacial structures, including the zygoma and nasal bone area, and widening of the circummaxillary sutures. Minor buccal tipping of the dentition was observed, but the integrity of the alveolar bone was preserved. This report demonstrates that careful design and application of the MARPE appliance can achieve successful transverse expansion of the maxilla and the surrounding structures in a patient beyond the age typically considered acceptable for traditional rapid palatal expansion.
Highlights
- •
We examined the effectiveness of a novel design for a microimplant-assisted rapid palatal expansion.
- •
We developed a standard protocol for microimplant-supported expansion.
- •
Implant-supported expansion offers vertical control and limits dental side effects.
- •
Orthopedic expansion is possible beyond the age previously thought possible.
Previous research has indicated that approximately 18% of mixed-dentition patients have a transverse maxillary constriction. Traditionally, they are treated with rapid palatal expansion (RPE) techniques that rely on a combination of orthopedic and dental expansion to correct the skeletal disharmony. Many types of RPE appliances have been developed with different rates of expansion, but the principles are essentially the same. By exerting a rapid transverse force on the maxillary dentition, the midpalatal suture is disrupted and separated, leading to increased cellular activity in that area that induces bone remodeling. Because conventional RPE appliances by design transmit the expansion forces through the teeth, alveolar bone bending and dental tipping are inevitable, particularly in older patients. Such movements not only take up a significant portion of the total activation of the device, reducing the true skeletal expansion, but also lead to clockwise rotation of the mandible and opening of the bite.
Recently, microimplant-assisted RPE (MARPE) appliances that can localize the lateral forces to the midpalatal suture while minimally using the dentition have become available for treatment of transverse maxillary constriction in older patients. However, the method to maximize the effects of the MARPE technique in clinical situations has not been thoroughly studied, and a standardized design or an expansion protocol has not been published. This case report illustrates the successful orthopedic correction of an adult before fixed orthodontic treatment. Elimination of the transverse skeletal discrepancy was achieved using a novel MARPE design and expansion protocol. Clinicians and researchers must continue to investigate the mechanism of successful MARPE treatment and establish an effective treatment protocol.
Diagnosis and etiology
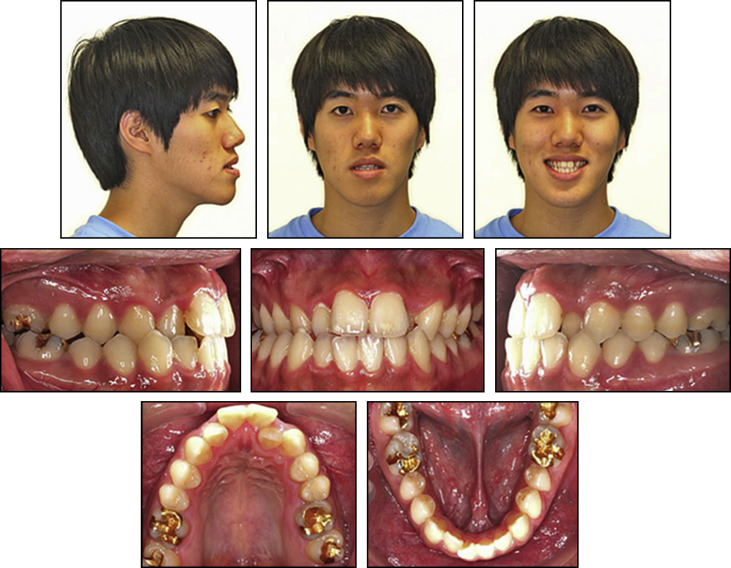
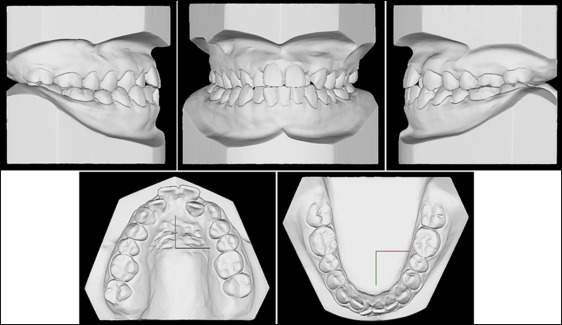
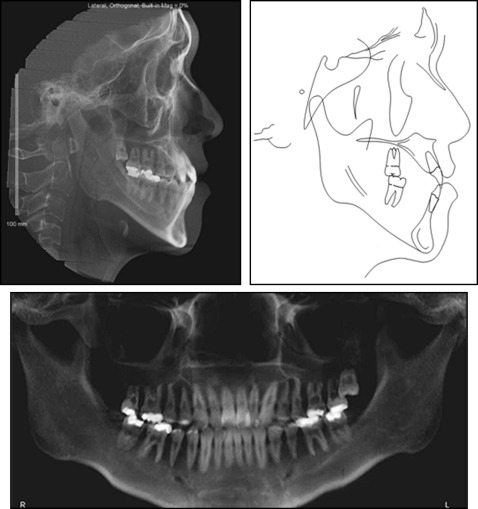
A Korean man, 19 years 4 months of age, came to the orthodontic clinic at the University of California, Los Angeles, for consultation and screening ( Figs 1-3 ). His chief complaint was “I have crowding in the front, and I am not happy with the arrangement of my teeth.” He had 6 mm of arch width discrepancy measured by the distance between the first molars accompanied by a unilateral crossbite of the right posterior dentition as well as 3 mm of mandibular dental midline and chin deviation to the same side. There were crowding amounts of 7 mm in the maxilla and 3 mm in the mandible. He had already had numerous orthodontic consultations and wanted to avoid any form of orthognathic surgery. There was no history of a family predilection for a Class III skeletal growth pattern.
Treatment objectives
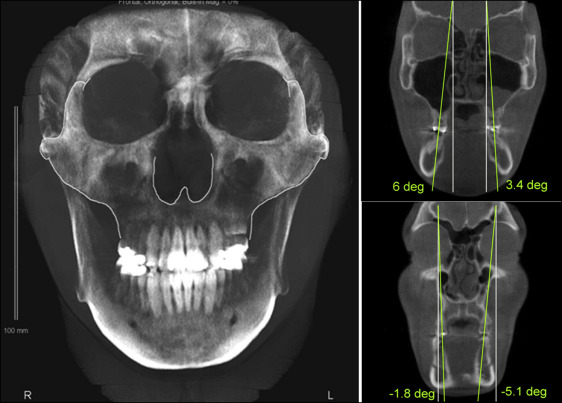
The patient had a unilateral posterior crossbite with dental compensation caused by a skeletal imbalance ( Fig 4 ). Since a harmonious occlusion could not be achieved with such a skeletal problem, the first objective of orthodontic treatment was orthopedic correction of the posterior crossbite, followed by fixed orthodontic treatment. Consistent with the amount of arch width discrepancy measured at the first molars, it was concluded that an increase of approximately 8 mm in the width of the basal structures was the goal for the expansion phase of this treatment. In this case report, we address mainly the effect of the expansion phase of treatment to highlight the importance of the MARPE protocol. These additional objectives of care were also included: (1) improve the facial profile and symmetry, (2) create ideal overbite and overjet, and (3) improve the dental and skeletal relationships in 3 planes of space.
Treatment objectives
The patient had a unilateral posterior crossbite with dental compensation caused by a skeletal imbalance ( Fig 4 ). Since a harmonious occlusion could not be achieved with such a skeletal problem, the first objective of orthodontic treatment was orthopedic correction of the posterior crossbite, followed by fixed orthodontic treatment. Consistent with the amount of arch width discrepancy measured at the first molars, it was concluded that an increase of approximately 8 mm in the width of the basal structures was the goal for the expansion phase of this treatment. In this case report, we address mainly the effect of the expansion phase of treatment to highlight the importance of the MARPE protocol. These additional objectives of care were also included: (1) improve the facial profile and symmetry, (2) create ideal overbite and overjet, and (3) improve the dental and skeletal relationships in 3 planes of space.
Treatment alternatives
A common treatment modality for correcting an arch width discrepancy caused by a constricted maxilla is conventional RPE. Because of the rigid, interdigitated form of the palate in adults, limited lateral and midline maxillary osteotomies can be combined with fixed palatal expanders for surgically assisted RPE. Other surgical methods such as a 3-piece LeFort I osteotomy can also be considered, especially if there is a skeletal disharmony in the anteroposterior or vertical dimension. However, these approaches involve more invasive procedures, with increased risks and costs for the patient.
Another option was to treat the patient entirely with dental movement. It has been suggested that the arch dimensions can be significantly increased by using fixed orthodontic appliances with light forces and reduced friction. However, such translational tooth movement and buccal bone remodeling have not been adequately described in previous studies.
All options were discussed with the patient, and he chose the MARPE approach to reduce the costs and potential surgical risks. Based on previous patients treated in our clinic, we believed that MARPE could provide an expansion force that separates the rigid midpalatal suture without the need for surgery. Additionally, the risks and costs are minimal compared with the surgically assisted RPE approach. In contrast to RPE, MARPE is advantageous because it directs expansion forces toward the midpalatal suture and away from the molars, resulting in more notable orthopedic correction and minimal tooth movement. An example of the MARPE appliance used for this patient is shown in Figure 5 .
Treatment progress
The MARPE expander was delivered with 4 microimplants (1.5 × 11 mm) inserted in the 1.5 × 2-mm slots of the appliance. The insertion slots ensure a precision fit with the microimplants and guarantee that the microimplants are in a secured perpendicular position. The 11-mm length was chosen by considering the 2-mm height of the insertion slots, the 1 to 2 mm of space between the appliance and the palatal surface, the 1 to 2 mm of gingival thickness, and a desired 5 to 6 mm of bone engagement at a minimum. This was intended to promote the bicortical engagement of the microimplants into the palate. The size of the jackscrew was chosen based on the maximum screw size that would fit in the palatal vault, while still allowing close adaptation of the appliance to the tissue surface between the maxillary first molars. This position was selected to apply lateral forces against the pterygomaxillary buttress bone, which is a major resistance factor in maxillary expansion. The expansion rate was selected based on protocol developed by Dr Won Moon through clinical experience with the MARPE appliance and was adopted by the orthodontic clinic at the University of California at Los Angeles ( Table I ).
| Age of the patient | Initial expansion rate | Expansion rate after opening of the diastema |
|---|---|---|
| Early teens | 3 turns/week | 3 turns/week |
| Late teens | 1 turn/day | 1 turn/day |
| Adults | 2 turns/day | 1 turn/day |
| Older patients (>30 years) | >2 turns/day | 1 turn/day |
The activation started with 2 turns per day for the first 2 weeks until a diastema appeared; activation was stopped when the patient reported some discomfort in the palate and nasal cavity areas, and headache. The pain was resolved after a short discontinuation of the activation, and the activation resumed at a rate of 1 turn per day. After 10 mm of MARPE expansion and uprighting of the molars, 6 mm of expansion was gained at the maxillary first molars, and concomitantly 7 mm was achieved at the maxillary canines. The progress cone-beam computed tomography (CBCT) image was taken on the day that the expansion was completed. After 3 months to stabilize the expansion, the following were observed: (1) maxillary crowding was resolved, (2) the anterior crossbite was eliminated, and (3) the midlines were coincident (confirming the previously suspected functional shift).
Maxillary and mandibular fixed appliances were direct bonded to “idealize” the occlusion. A temporary anchorage device was placed between the maxillary right first and second premolars to slightly protract the maxillary right buccal segment. Finishing was completed with 0.017 × 0.025-in stainless steel archwires. The maxillary left third molar was then extracted ( Fig 6 ).
Treatment results
When the expansion was done, the upper craniofacial structures, including the maxillary basal bone, were noticeably widened ( Fig 7 ), leading to complete elimination of the crossbite. The preoperative and postoperative 2-dimensional radiographs and 3-dimensional CBCT images showed the observed expansion changes. The measurements show a relatively uniform increase in the width not only of the alveolar area, but also in the upper maxillofacial structures such as the zygoma and nasal bone ( Table II ; Fig 8 ). The first molars and premolars showed slight increases in buccolingual angulation ( Table III ). The effect of the expansion also measured on the dental casts showed an overall width increase of 6 mm in the maxillary arch that was maintained throughout the retention period ( Fig 9 ). The patient finished treatment with Class I molar and canine relationships ( Fig 10 ).
| Width | Initial (mm) | Removal of the expander (mm) | Gain of width (mm) | Final (mm) | Gain of width (mm) |
|---|---|---|---|---|---|
| Basal bone | 59.7 | 65.8 | 6.1 | 65.8 | 6.1 |
| Zygomatic bone | 110.3 | 116.0 | 5.7 | 114.7 | 4.4 |
| Nasal cavity | 29.9 | 33.7 | 3.8 | 33.7 | 3.8 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


