Crestal implants
BOI implants
Clinical advantages
Threaded pin/vertical aspect of the implant
Surface-enlarged:
– Macrodesgn: thread
– Etching/sandblasting
Machined surface
BOI implants are less infection-prone
Load transmission
Vertical; dose to or far from the mouth depending an the design
Basal, far from the mouth
Load transmission area in infection-protected regions
Structure of the load-bearing areas
Pole near the core
Broad lateral support
Load transmission vs. infection
Load transmission areas roughly coincide with infection entry paths
Load transmission areas are removed from infection entry paths
BOI implants are less infectionprone
Nutrient and oxygen supply
Enossal supply of nutrients and transport speed are limited
Periosteal supply of nutrients can be regulated within wide margins
Overload situations can be caught and repaired by increasing the nutrient supply
Mucosal emergence point
Should be located in attached mucosa if the vertical aspect has a rough texture
May be located in either attached or unattached mucosa
Much freedom in positioning BOI implants; wounds may be closed with widely mobilized flaps after extractions
Synchronization of bone and superstructure
Restoration is synchronized with crestal/alveolar aspect of the bone due to rigid connection
Restoration is synchronized with basal aspect of the bone due to rigid connection
The fate of the alveolar bone is of no consequence for the preservation of BOI implants; large bridges synchronize basal bone areas; horizontal and vertical BOI aspects, interfaces compensate for any lack of synchronicity
Recall requirements
Frequent
Less frequent than for natural teeth
Low cost to patients during the maintenance phase; treatment success not very dependent on hygiene
Nicotine abuse
Influences the implant’s chance of survival
Influences only the initial soft-tissue healing process
Smoking is no contraindication; it only constitutes a risk during initial wound healing
Implant volume
Screw 5×13 mm: 200 mm2
EDS 9G9: 67 mm2
Better blood supply to the implant side. Better passage from blood through the implant site
Volume of bacteria and debris in a 2 mm pocket (assuming the layer is 0.01 mm thick)
Diameter Volume 3.75 mm 0.24 mm3 4.8 mm 0.30 mm3
Diameter Volume 1.9 mm 0.12 mm3
Thin penetration areas show less debris and significantly less bacterial attack surface. Less bacteria-related changes of blood flow in direction and quantity
Abutment diameter
3.3–6.5 mm
1.9–2.3 mm
Infection repelled “on all sides”
We believe the reason to be the implant design and the nature of the insertion process. Table 8.1 shows the differences between crestal and BOI implant types and the clinical advantages of the latter.
It should be noted that the differences are shown and organized here in terms of general principles. Certain types of crestal implants do not quite fit the pattern. Various transitional types exist:
-
The bicortical screw (Oraltronics) with its very wide thread combined with smooth vertical implant surfaces is one of these exceptions. This implant is strictly basally osseointegrated even though it is inserted from crestally.
-
The so-called porous-coated implants (such as Osseopore) are another of those exceptions. With their large perfusion areas located close to the implants, they offer a three-dimensional nutrient matrix to the cortical bone. By contrast with conventional screw implants, the implants can be short and still afford firm and stable anchorage. A disadvantage of this type of implant is that they are extremely prone to infection during the healing phase, since the perfusion areas, which are located in the depth of the three-dimensional structure, are rapidly colonized and offer a favourable environment for bacterial growth. Once colonized, these areas are practically impossible to sanitize. Once integrated, on the other hand, Osseopore implants are extremely durable. Longer implants with the same type of surface are less suitable, since the perfusion paths, reaching from basally to crestally, become too long and impenetrable, ultimately eliminating the advantages these implants otherwise offer.
-
Crestal implants with a conical design are another peculiar type: Compression screws with a pronounced conical shape do not offer enough contact area for deep enossal load transmission. Since the osseointegrated implant surface increases toward the crestal aspect, direct interaction between this surface and the cortical bone will also increase in quantitative (relative) terms. Compared to cylindrical screws, a smaller percentage of the load is transmitted in the basal part of the bone and a greater percentage in the crestal part with these implants. This aspect probably helps these implants promote bone preservation. Since remineralization tends to be more pronounced in the crestal area, these implants are more resistant to infection than are cylindrical screws.
There is a considerable difference between this procedure and established ideas concerning the succession of periodontal therapy and prosthodontic therapy. What is true of teeth is usually not valid for complete dentures supported by BOI implants.
Since BOI implants permit immediate insertion of fixed restorations throughout the treated region, it is not necessary to perform periodontal therapy before the extraction of teeth and the insertion of implants. This means that the excellent local blood supply of the intraoral soft tissues can be used to advantage. This means that the chances of effective postoperative infection control are greatly enhanced. With crestal implants, the implant itself blocks the most effective path of removal for intraoperatively introduced inflammatory processes and their residue, while BOI implants always allow efficient suppuration through the insertion slots.
As a rule, long-term provisional restorations will be inserted following BOI therapy, especially in the maxilla. Any gingival shrinkage or bone remodelling that does occur will be of no practical consequence. Aesthetics are restored once the soft tissues have healed – that is, at a time when the mucosal situation will have stabilized.
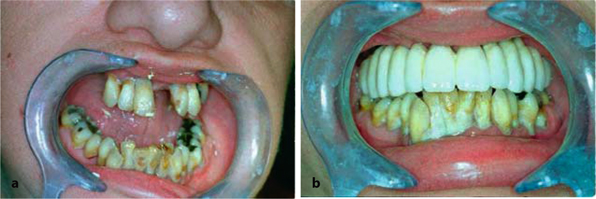
Fig. 8.1a,b.
This 40-year-old patient was primarily interested in a more beautiful maxillary smile. Her mandibular teeth were barely visible when she opened her mouth normally. For this reason (and probably also for financial reasons) the maxilla was to be selectively treated. The mandibular teeth were simply cleaned (which has no long-term effect). One year postoperatively, the mandibular situation was just as desolate as before treatment. The extreme build-up of concrements with extensive bacterial plaque did not influence the positive healing process of the implants, whose threaded pins did not show any plaque or calculus
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


