Introduction
The aims of this study were to identify a sample of borderline Class I extraction and nonextraction patients and to investigate posttreatment changes in arch-width and perimeter measurements.
Methods
A parent sample of 580 Class I patients was subjected to discriminant analysis, and a borderline subsample of 62 patients, 31 treated with extraction of 4 first premolars and 31 treated without extractions, was obtained. The patients’ plaster casts were digitally scanned, and the maxillary and mandibular intercanine and intermolar widths and perimeters were assessed.
Results
The extraction group showed increases in maxillary and mandibular intercanine widths ( P <0.001) and decreases in mandibular intermolar width and in maxillary and mandibular perimeters ( P <0.001). The nonextraction group showed increases in all 4 arch-width measurements ( P ≤0.003), whereas the maxillary and mandibular perimeters were maintained. The posttreatment differences between the 2 groups showed significant differences in the maxillary ( P <0.001) and mandibular intermolar widths ( P <0.001). Also, the comparison of the arch perimeters between the 2 treatment groups showed adjusted differences of −8.51 mm ( P <0.001) and −8.44 mm ( P <0.001) for the maxillary and mandibular arches, respectively. The intercanine widths showed no changes between the 2 treatment groups.
Conclusions
Borderline Class I patients treated with extraction of 4 first premolars had decreased maxillary and mandibular intermolar and perimeter measurements compared with nonextraction patients. The maxillary and mandibular intercanine widths showed no significant difference between the 2 treatment groups.
Highlights
- •
Discriminant analysis identified borderline extraction and nonextraction patients.
- •
Perimeter curves were drawn on a constructed occlusal plane.
- •
Extractions led to a transverse dental arch decrease posteriorly.
- •
Nonextraction dental arches showed an increase of all arch-width measurements.
- •
Perimeter curves decreased in extraction and were maintained in nonextraction patients.
In planning treatment for a patient, an experienced orthodontist reaches a decision in regard to the extraction or nonextraction treatment modality. In clear-cut cases, the decision is easy to make; however, some patients can be treated either way, forcing the orthodontist to deliberate between different treatment options. These borderline patients require a careful estimate of the possible impact of the treatment choice on the facial profile, smile esthetics, stability, and other factors that the orthodontist considers in favoring 1 treatment option over another.
Often, concerns arise about the impact of the extractions on soft tissue esthetics. McNamara reported a direct link between arch width and smile esthetics, whereas Zachrisson indicated that the inclinations of the canines and premolars are a key factor for a full smile. Recently, changes in buccal corridors have been compared after extraction and nonextraction treatments. Although a minimal buccal corridor is favorable, extraction therapy does not necessarily lead to a smaller arch width than nonextraction therapy. Some authors have reported widening of the maxillary intercanine width in extraction patients, but Germeç-Cakan et al found no significant change. A slight increase regarding mandibular intercanine width has been reported in extraction patients. On the other hand, intermolar width seems to decrease during extraction treatment in both jaws.
In retrospective surveys that compare outcomes of treatment modalities, all groups must be equally matched according to the diagnostic variables that the clinician uses to establish a treatment decision. In orthodontics, these variables are the measurements of the cephalometric analysis and the dental casts along with the patient’s age and sex. However, the majority of the aforementioned studies assessed treatment changes either in clear-cut or in arbitrarily defined borderline cases in regard to the extraction modality. Furthermore, several studies included different types of malocclusion in the same treatment group. Inevitably, the results of those studies were often contaminated with susceptibility bias, defined as the difference in prognostic expectations from preexisting differences at the onset of treatment. Such patient’s features that lead a clinician to a specific treatment decision are called confounding variables. Discriminant analysis is a statistical multivariate technique that deals concurrently with a large number of confounding variables.
In current orthodontic research, discriminant analysis has been proven to mimic the decision-making process of an experienced orthodontist. This analysis can predict group membership, as in extraction or nonextraction treatment. It can also identify a spectrum of borderline patients who cannot be classified to any group and consequently could be treated either way. The use of discriminant analysis ensures that all patients who comprise the borderline group are equally susceptible to both treatment modalities; therefore, susceptibility bias is eliminated.
The aims of this study were to identify a bias-free sample of extraction and nonextraction Class I patients and to compare their transverse maxillary and mandibular arch-width and perimeter changes.
Material and methods
A parent sample of 580 patients (349 female, 231 male) was collected from the graduate orthodontic clinic of the School of Dentistry of the National and Kapodistrian University of Athens, Greece and 5 private orthodontic practices in Athens, Greece. Of these patients, 427 received nonextraction treatment, and 153 were treated by extraction of the 4 first premolars.
All patients were white, with a full complement of teeth (excluding the third molars) and a Class I dental and skeletal malocclusion. They had no history of cleft, dentofacial deformity, or syndrome, and they also had never received orthodontic or orthognathic surgery treatment. All patients were treated with preadjusted edgewise appliances in both arches, without the use of any extraoral or temporary anchorage device. The patients’ diagnostic records included an initial lateral cephalometric radiograph taken in natural head position, a panoramic radiograph, and initial and final dental casts. All cephalometric analyses were performed using Viewbox (version 4.0.1.7; dHAL Software, Kifissia, Greece). The research protocol was approved by the ethics committee of the National and Kapodistrian University of Athens, Greece.
To eliminate proficiency and selection bias, the parent sample was reduced to a borderline sample by means of a stepwise discriminant analysis. The confounding variables used in the discriminant analysis were 26 cephalometric and 6 plaster cast measurements along with the 2 variables of sex and age. This approach allowed an accurate representation of the most important dental, skeletal, and soft tissue traits that have an impact on an orthodontist’s treatment decision. A discriminant score was calculated for each patient ranging from −3.5 to +3.07. Although patients with positive scores were most likely treated without extractions, patients with negative scores received extraction treatment. The unclassified patients around the cutoff point, determined at 0, were identified as the borderline subjects and composed the borderline spectrum.
Finally, a group of 62 Class I borderline patients (38 female, 24 male) who exhibited similar degrees of dental and skeletal discrepancies at the onset of treatment was identified. Of these patients, 31 were treated nonextraction, and 31 were treated by extraction of the 4 first premolars. Of the nonextraction patients, 17 (54.84%) were female, and 14 (45.16%) were male. Of the extraction patients, 21 (67.74%) were female, and 10 (32.26%) were male. The mean ages were 14.0 years (SD, 5.44) for the nonextraction and 13.0 (SD, 3.27) for the extraction groups, respectively.
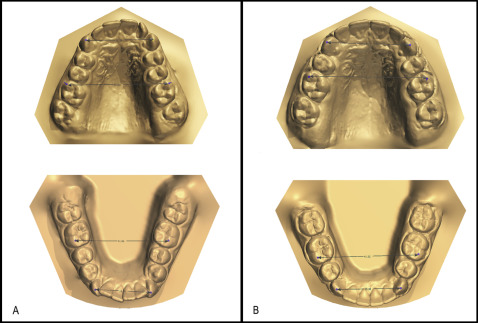
Next, to measure the maxillary and mandibular intercanine and intermolar widths and arch perimeters, the pretreatment and posttreatment plaster dental casts of the borderline patients were used. All dental casts were scanned with a digital scanner (3Shape R700; 3Shape, Copenhagen, Denmark), and the measurements were performed with Ortho Analyzer software (3Shape 2013-1; 3Shape, Copenhagen, Denmark). The intercanine width was assessed as the distance between the cusp tips of the maxillary and mandibular right and left canines, and the intermolar width was assessed as the distance between the mesiobuccal cusp tips of the right and left first molars in the maxillary and mandibular arches ( Fig 1 ).
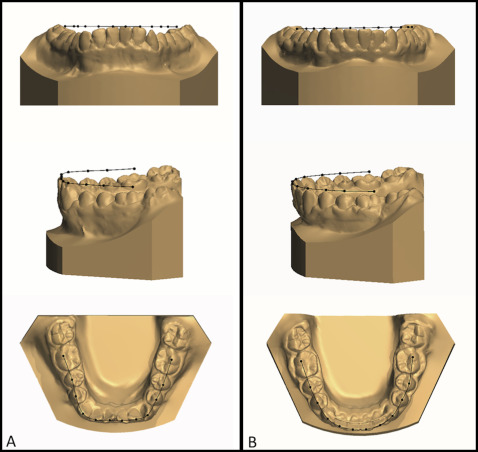
Additionally, to assess the arch perimeter more accurately, we created a constructed occlusal plane for each arch by projecting 3 points above the actual occlusal plane. These projected points that defined the constructed occlusal plane were derived from a point at the incisal tip of the right central incisor, a point at the mesial buccal cusp of the right first molar, and a point at the mesial buccal cusp of the left first molar for the maxillary and mandibular arches, respectively. Then a specific point from each tooth up through the first molars (12 teeth) was projected on the constructed occlusal plane as follows: a point at the middle of the incisal edge of the 4 anterior incisors, a point at each buccal cusp of the first and second premolars, and a point at the distobuccal tip of the first molar. Next, the projected points were connected and formed the perimeter curves of each dental arch for the maxilla and the mandible ( Fig 2 ).
To assess the intragroup and intergroup differences in transverse arch changes, descriptive and inferential statistics were performed. The mean differences that each treatment group experienced from pretreatment to posttreatment were also compared using independent sample t tests. Additionally, paired t tests were calculated to assess the differences between the pretreatment and posttreatment measurements for the 2 groups. Since the dependent variables were likely to be correlated, multivariate regression analysis was used to adjust the P values for multiple comparisons using F tests. The significance level was predetermined at 5%.
All measurements were performed by the principal investigator (C.H.). Additionally, evaluations were performed for both random and systematic errors of the method. To assess intraexaminer repeatability, with a table of random numbers, 20 subjects were selected—10 from each group—and were reevaluated 3 weeks later by the same investigator. Also, to assess interexaminer agreement, 20 subjects—10 extraction and 10 nonextraction—were randomly selected, and the principal investigator was evaluated against another examiner (D.K.). This examiner was a member of the National Board of Orthodontics of Greece.
The intraclass correlation coefficient (ICC) based on the variance components from a 1-way analysis of variance was used. The results showed excellent agreement: ICC, 0.99; 95% confidence interval (CI), 0.99-0.99 for intraexaminer agreement; and ICC, 0.98; 95% CI, 0.95-0.99 for interexaminer agreement. Statistical analysis was carried out using SPSS software (version 19.0; IBM, Armonk, NY).
Results
The descriptive statistics for the morphologic characteristics of the borderline sample are listed in Table I . In regard to the arch-width measurements, the descriptive characteristics of the 2 groups of patients are listed in Table II . The P values ( t test for independent samples) of the borderline sample measurements showed no statistically significant differences between the extraction and nonextraction patients at the onset of treatment. This finding was further confirmed by the P value of 0.321 for pretreatment differences in all outcomes.
| Nonextraction | Extraction | P value ∗ | |
|---|---|---|---|
| Cephalometric variables | |||
| SNA (°) | |||
| Mean | 82.26 | 82.21 | 0.965 |
| SD | 3.07 | 4.22 | |
| SNB (°) | |||
| Mean | 78.34 | 78.52 | 0.836 |
| SD | 2.67 | 3.68 | |
| ANB (°) | |||
| Mean | 3.81 | 3.63 | 0.758 |
| SD | 2.26 | 2.17 | |
| FMIA (°) | |||
| Mean | 63.39 | 62.18 | 0.113 |
| SD | 5.64 | 4.13 | |
| IMPA (°) | |||
| Mean | 91.33 | 92.32 | 0.102 |
| SD | 5.72 | 5 | |
| FMA (°) | |||
| Mean | 25.28 | 25.38 | 0.129 |
| SD | 4.43 | 3.94 | |
| U1-SN (°) | |||
| Mean | 105.31 | 103.34 | 0.366 |
| SD | 8.44 | 7.14 | |
| U1-NA (°) | |||
| Mean | 22.80 | 20.91 | 0.389 |
| SD | 8.43 | 7.26 | |
| U1-NA (mm) | |||
| Mean | 4.00 | 3.72 | 0.716 |
| SD | 2.99 | 2.70 | |
| L1-NB (°) | |||
| Mean | 25.82 | 26.57 | 0.497 |
| SD | 3.21 | 4.55 | |
| L1-NB (mm) | |||
| Mean | 5.07 | 4.70 | 0.527 |
| SD | 2.03 | 2.15 | |
| Z angle (°) | |||
| Mean | 72.01 | 73.07 | 0.480 |
| SD | 5.47 | 5.42 | |
| N-Me (mm) | |||
| Mean | 110.35 | 110.80 | 0.857 |
| SD | 6.68 | 10.79 | |
| N-ANS (mm) | |||
| Mean | 49.01 | 47.97 | 0.374 |
| SD | 3.76 | 4.72 | |
| ANS-Me (mm) | |||
| Mean | 63.32 | 65.00 | 0.308 |
| SD | 4.85 | 7.08 | |
| LL-E-plane (mm) | |||
| Mean | −0.30 | −0.48 | 0.814 |
| SD | 3.41 | 2.53 | |
| Model variables | |||
| Overbite (mm) | |||
| Mean | 2.73 | 2.90 | 0.733 |
| SD | 1.60 | 1.89 | |
| Overjet (mm) | |||
| Mean | 2.32 | 2.08 | 0.576 |
| SD | 1.96 | 1.02 | |
| Maxillary crowding (mm) | |||
| Mean | −2.51 | −2.93 | 0.448 |
| SD | 2.71 | 1.16 | |
| Mandibular crowding (mm) | |||
| Mean | −4.95 | −5.37 | 0.164 |
| SD | 1.13 | 1.07 | |
| Characteristic | Extraction (n = 31) | Nonextraction (n = 31) | P value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Maxillary intercanine width (mm) | |||
| Pretreatment | 33.32 ± 2.62 | 33.63 ± 1.87 | 0.602 |
| Posttreatment | 35.22 ± 1.89 | 35.25 ± 1.22 | 0.930 |
| Mandibular intercanine width (mm) | |||
| Pretreatment | 25.64 ± 2.56 | 25.69 ± 1.79 | 0.923 |
| Posttreatment | 27.04 ± 1.27 | 26.89 ± 1.11 | 0.619 |
| Maxillary intermolar width (mm) | |||
| Pretreatment | 49.01 ± 3.50 | 50.51 ± 2.40 | 0.056 |
| Posttreatment | 48.32 ± 2.44 | 52.07 ± 1.94 | 0.000 |
| Mandibular intermolar width (mm) | |||
| Pretreatment | 43.11 ± 3.78 | 44.14 ± 2.61 | 0.219 |
| Posttreatment | 41.39 ± 2.61 | 45.42 ± 2.05 | 0.000 |
| Maxillary arch perimeter (mm) | |||
| Pretreatment | 93.34 ± 5.54 | 93.09 ± 4.22 | 0.847 |
| Posttreatment | 84.42 ± 6.71 | 92.75 ± 5.82 | 0.000 |
| Mandibular arch perimeter (mm) | |||
| Pretreatment | 80.20 ± 5.36 | 81.46 ± 5.70 | 0.378 |
| Posttreatment | 72.47 ± 6.92 | 81.62 ± 5.80 | 0.000 |
| Age at baseline (y) ∗ | 13.0 (±3.27) | 14.0 (±5.44) | 0.474 |
| Sex | 0.297 | ||
| Male (%) | 10 (32.26) | 14 (45.16) | |
| Female (%) | 21 (67.74) | 17 (54.84) | |
When we compared the 2 treatment groups, the differences of the mean change values for the maxillary and mandibular intercanine widths did not show any statistically significant difference. Contrariwise, the differences of the mean change values for the maxillary (adjusted mean difference, −2.66; 95% CI, −3.68 to −1.65; P <0.001) and mandibular (adjusted mean difference, −3.42; 95% CI, −4.52 to −2.32; P <0.001) intermolar widths were statistically significant. The comparison of the arch perimeters between the 2 treatment groups showed adjusted differences of −8.51 mm (95% CI, −11.62 to −5.40; P <0.001) and −8.44 mm (95% CI, −11.47 to −5.41; P <0.001) for the maxillary and mandibular arches, respectively. However, the overall P value between the mean changes of the 2 treatment groups was statistically significant (overall P value <0.001) ( Table III ).
| Difference between pretreatment and posttreatment measurements | Extraction (95% CI) | Nonextraction (95% CI) | Adjusted difference ∗ (95% CI) | P value | Overall P value † |
|---|---|---|---|---|---|
| <0.001 | |||||
| Maxillary intercanine width (mm) | 1.90 (1.21, 2.59) | 1.63 (0.94, 2.32) | 0.09 (−0.91, 1.10) | 0.852 | |
| Mandibular intercanine width (mm) | 1.40 (0.71, 2.10) | 1.20 (0.50, 1.89) | 0.05 (−0.96, 1.06) | 0.920 | |
| Maxillary intermolar width (mm) | −0.69 (−1.44, 0.06) | 1.57 (0.82, 2.32) | −2.66 (−3.68, −1.65) | <0.001 | |
| Mandibular intermolar width (mm) | −1.72 (−2.54, −0.90) | 1.28 (0.47, 2.10) | −3.42 (−4.52, −2.32) | <0.001 | |
| Maxillary arch perimeter (mm) | −8.92 (−11.05, −6.78) | −0.34 (−2.48, 1.79) | −8.51 (−11.62, −5.40) | <0.001 | |
| Mandibular arch perimeter (mm) | −7.74 (−9.89, −5.58) | 0.15 (−2.00, 2.31) | −8.44 (−11.47, −5.41) | <0.001 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


