This clinical article reports a technique, apicotomy, for managing dilacerated or ankylosed canines. The records of 3 patients successfully treated with apicotomy are presented. Orthodontists observe clinically significant incidences of impacted maxillary canines in their daily practices. Several procedures have been described to bring an ankylosed, impacted tooth into occlusion. Luxation is the most widely used solution, but there are risks involved with that approach, and the success rate is low. Surgical repositioning has also been used, but morbidity is high, and the aggressiveness of the procedure might also contraindicate it. Ankylosis might be related to the anatomic position of the canine’s root apex and its adjacent anatomic structures. Apicotomy is a guided fracture of a canine root apex, followed by its orthodontic traction. It is a conservative surgical alternative for treating impacted canines with dilacerations or apical root ankylosis.
Excluding the third molars, the maxillary canines are the most commonly impacted permanent teeth, with impaction occurring more frequently in female patients than in males with a proportion of 2.5:1. The theories of canine impaction include the distance they must travel to reach the occlusion, arch-length discrepancy, alveolar bone condensation, root dilaceration, and any form of ankylosis. The crown of impacted canines can be located labially or palatally but is most often palatal. Asians have a significant number of labial impactions.
Occasionally, while attempting to bring an impacted tooth into proper occlusion, a clinician can be confronted with no response, and the first sign of ankylosis is frequently the intrusion of adjacent teeth. Dentoalveolar ankylosis is an anomaly of eruption that involves anatomic fusion of the alveolar bone with the cementum or dentin.
Five treatment options for impacted maxillary canines are commonly considered: long-term monitoring, interceptive removal of the deciduous canine to aid in the eruption of the permanent successor, surgical removal of the impacted canine, surgical exposure with orthodontic traction and alignment, and autotransplantation of the impacted canine. It has been suggested that the treatment time for a malocclusion with an impacted canine might be longer than a similar malocclusion in which all teeth have erupted. Much depends upon the tooth’s position, eruption pattern, and stage of root formation.
Based on an investigation of impacted teeth, Puricelli observed that the ankylosis might be related to the anatomic position of the canine’s root apex and its adjacent anatomic structures. Puricelli has developed and described a surgical technique called apicotomy , a conservative intervention for impacted canines with dilacerations or apical root ankylosis. The diagnosis of apical root ankylosis is generally related to the position of the canine apex with the anatomic structure known as the inverted Y of Ennis. This structure is defined as the region where the cortices of the nasal cavity and the maxillary sinus meet.
The purpose of this article is to describe the technique and illustrate it with the records of 3 patients to demonstrate the retrieval of dilacerated or ankylosed maxillary canines.
Procedure
An apicotomy is a guided fracture of a canine root apex performed with a small chisel followed by orthodontic traction of the canine crown. The canine apex is surgically exposed, and a groove is made on the root with a small round dental bur, defining the place where the chisel should be placed for fracturing the root apex. The procedure has been successfully tested. Puricelli’s data showed that in 29 patients who had the procedure, 26 procedures were successful and 3 failed. In cases of failure, the canine must be extracted and another solution used.
A week after surgery, orthodontic traction should be applied with a force of approximately 100 g. A vertical direction of pull is preferred but not always possible. Ballista loops on round stainless steel 0.018-in wires have been shown to be effective. As the case progresses, the force can be slightly increased. The force should be monitored every 2 weeks because long periods without activation can lead to new ankylosis. Radiographic examinations are recommended at the start and again at 2 and 4 weeks. It is important to observe that the root tip is fractured and left in place to increase the chances of the tooth’s remaining vital. Pulp tests should be performed after 3 months; in a significant number of patients, the tooth remains vital. Figures 1 through 11 illustrate the timing and the success of the apicotomies in 3 patients.

Patient 1, a 14-year-old white boy, presented for treatment at the Saint Louis University in St Louis, Mo. His medical history showed that he had type I diabetes, which was considered during treatment planning. The patient had a Class I malocclusion with significant crowding of the maxillary arch and an impacted maxillary left canine ( Fig 1 ). After examining all records, it was decided to try to treat this patient without extractions. The patient had much growth left, and his dentition could very well develop into a Class III pattern. The treatment protocol included gaining space for the impacted canine, surgical exposure, and bonding of an attachment to bring the tooth into occlusion. The space between the lateral incisor and the first premolar was opened orthodontically. The closed-eruption surgical exposure technique of the canine was used, and traction was initiated ( Fig 2 ).
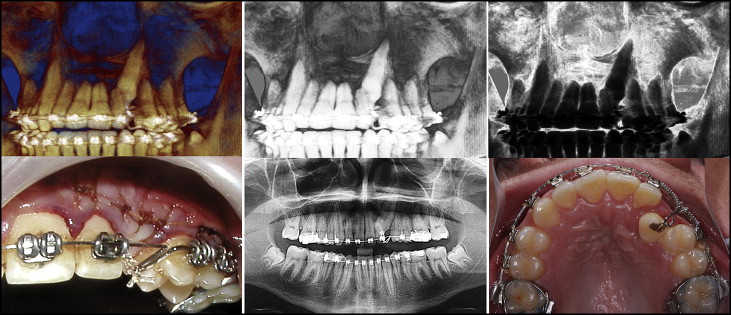
After 3 months, a bite opening on the left side was noted, with no movement of the canine. These signs suggested ankylosis. The patient’s mother had an ankylosed canine, which had been extracted. The apicotomy procedure was explained to the patient and his family, and the decision was made to proceed with it. The surgery was done, and the canine traction was started after 1 week. A ballista loop was used initially. Six weeks later, the canine was erupting, and the traction was continued. After 10 weeks, the canine had been totally erupted, and its rotation and alignment in the arch had begun. The case was completed and the tooth was tested vital; after removal of the fixed appliance, recontouring of the gingiva was suggested for better esthetics. The final intercuspation and the torque of the impacted canine could have been better ( Fig 3 ), but because the treatment had lasted too long and the patient’s general health condition had worsened with his diabetes, the appliances were removed.

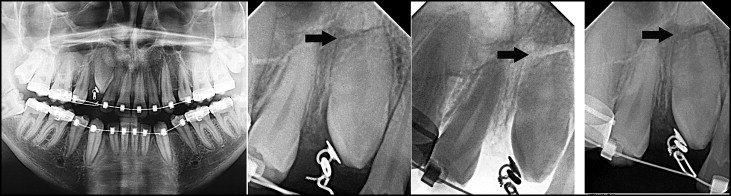
Patient 2 is a 22-year-old black man. He presented for treatment at Saint Louis University in St Louis, Mo. The records showed a Class I malocclusion with severe crowding. All teeth were present except the maxillary right canine. The maxillary right deciduous canine was still present ( Fig 4 ). The impacted maxillary right canine was palatally positioned in relation to its deciduous predecessor. The treatment plan called for extraction of the maxillary and mandibular first premolars; they were extracted along with the maxillary right deciduous canine. Treatment progressed with the expectation that the impacted canine would erupt by itself. It did not, so the tooth was exposed, and traction was applied to bring it into alignment. Unfortunately, the canine did not move. The patient at this time already had the 4 premolars extracted, and the possibility of ankylosis of the maxillary right canine was evident ( Fig 5 ).

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


