Introduction
The purpose of the study was to evaluate impacted maxillary canines as risk factor for orthodontic apical root resorption.
Methods
The sample comprised 66 patients treated with fixed appliances. Thirty-two patients with a unilateral impacted maxillary canine, which was distanced from the roots of the incisors at a preliminary phase of treatment before bonding, formed the impaction group, and 34 patients without impactions served as the controls. Root shortening was calculated by using pretreatment and posttreatment intraoral radiographs. Inclination of the eruption path of the impacted canine relative to the midline, axis of the lateral incisor, and nasal line, root development, and the medial and vertical positions of the impacted tooth were recorded on orthopantomograms and lateral cephalometric films. The follicle/tooth ratio was evaluated by using periapical radiographs.
Results
No significant difference in apical resorption of the maxillary incisors was detected between the impaction and control groups, or between the incisors of the impacted and contralateral sides in the same subject. Likewise, no difference in the severity of root resorption was found between the incisors of impacted side alone and the incisors of the control group. Mesial and vertical inclinations of the impacted canines were negatively related to a lateral incisor’s root resorption. No correlations were found between resorption and medial or vertical position of the crown of the canine. The follicle/tooth ratio was significantly related to the mesial inclination of the impacted canine, but not to root resorption.
Conclusions
An impacted maxillary canine, after being distanced from the incisor roots, does not seem to be a risk factor for apical root resorption during orthodontic treatment.
The maxillary permanent canine is the tooth that most commonly fails to erupt after the third molars. The reported incidence of impacted maxillary canines varies between 0.9% and 2.9%. It is speculated that in any orthodontic practice the incidence might be as high as 23.5%. Eighty-five percent of impacted canines are located palatally to the line of the arch. Stivaros and Mandall reported palatal and labial canine impaction in 61% and 5% of patients, respectively. The remaining 34% were located in the middle of the alveolar bone buccopalatally.
The most common problem caused by impacted canines is resorption of the roots of the adjacent lateral incisors. With plane film radiography, this incidence was found to be less than 10% of the patients affected. Ericson and Kurol, using polytomography and intraoral radiographs, found that lateral incisor root resorption occurred in approximately 12% of the patients with impacted maxillary canines. However, using computerized tomography (CT) of the maxillae in a sample of 107 children with ectopically erupting canines, the same authors found resorption in 38% of the maxillary lateral incisors and 9% of the central incisor roots, whereas 3% of the patients with normally erupting maxillary canines had root resorption of the lateral incisors. A study with cone-beam CT showed even higher incidences for root resorption (66.7% for lateral incisors and 11.1% for central incisors). CT scanning has also been valuable in determining the exact position of a malpositioned maxillary canine.
Correction of impacted maxillary canines often requires laborious orthodontic treatment, involving surgical exposure and orthodontic movement over a long distance to achieve proper alignment in the dental arch. The surgical and orthodontic procedures can increase the risks of gingival recession, bone loss, pulpal damage, and apical root resorption. The term “orthodontically induced inflammatory root resorption” has been proposed to describe the phenomenon of tooth structure loss during treatment. Inflammation, which is essential to tooth movement, is also known as a fundamental part of the root-resorption process. Several possible etiologic factors for root resorption have been identified: genetics, trauma, infections, and certain habits, but no clear causal relationship has been established.
Impacted maxillary canines have been shown to be risk factor for apical root resorption of the maxillary incisors during orthodontic treatment. Additionally, comparing the posttreatment root lengths of the incisors between the impacted and nonimpacted sides of patients with unilateral impactions, Woloshyn et al and Schmidt and Kokich found shorter roots on the impacted sides. An indication for no relationship between impacted canines and orthodontic root shortening of the adjacent teeth was given by Mavragani et al, while examining several factors affecting apical root resorption. However, the sample was not adequate, since the study was not designed to investigate this parameter.
It has been considered to be of high scientific and clinical interest to conduct a study to evaluate impacted canines as a risk factor for orthodontically induced inflammatory root resorption. Therefore, the specific aim of this investigation was to examine the effect of maxillary canine impaction on the severity of apical root resorption of the maxillary incisors during orthodontic treatment, after distancing the impacted canine from the incisor roots and eruption. Furthermore, the influence of the radiographic pretreatment characteristics of the impacted teeth on root shortening of the maxillary incisors was evaluated in relation to their posttreatment lengths.
Material and methods
This study was retrospective in design. The protocol was approved by the research ethical committee of the University of Bergen and the Norwegian Social Science Data Services. The sample comprised 66 subjects who had been treated with fixed appliances in the Postgraduate Clinic, Department of Clinical Dentistry, Orthodontics and Facial Orthopedics, at the University of Bergen in Norway. The data included pretreatment and posttreatment orthodontic documentation: complete diagnostic and treatment records, orthopantomograms, lateral cephalometric radiographs, and standardized intraoral periapical radiographs. The periapical radiographs were taken with the long-cone paralleling technique.
Among the 66 subjects, 32 (20 female, 12 male) had unilaterally impacted maxillary canines (impaction group). The mean age of the impaction group was 13.9 years (SD, 5.23; range, 10.0-33.4 years). Thirty-four patients with normally erupting canines (21 female, 13 male) with a mean age of 13.4 years (SD, 5.43; range, 9.8-35.0 years) were used for comparison (control group). A number of variables were recorded for each patient (sex, age, ANB angle, overjet, overbite, trauma of each incisor, habits, invagination of each incisor, agenesis, Class II elastics, extractions, root-form deviations of each incisor, late tooth shedding, body build, general factors, hormonal imbalances, allergies, treatment duration, and contraction duration). Among the 32 impacted canines, 23 (71.9%), 5 (15.6%), and 4 (12.5%) teeth were located palatally, buccally, and centrally, respectively. Eighteen were impacted on the right side and 14 were impacted on the left side.
Treatment of impacted maxillary canines in the Postgraduate Clinic at the University of Bergen is performed according to the following guidelines. The impacted canine is surgically exposed, and usually an attachment is placed for its traction. A transpalatal arch, with a finger spring attached to it, is used for canine traction ( Fig 1 ). When the canine has erupted, the patient is treated with fixed appliances.

Preoperative orthopantomograms and lateral cephalometric radiographs were randomly viewed and examined according to the methods of Ericson and Kurol and Power and Short. Digital radiographs were imported in SIDEXIS neXt Generation (version 1.51; Sirona Dental Systems, Bensheim, Germany) digital image system for measurements. Nondigitized radiographs were scanned (Expression 1680 scanner; Epson, Suwa, Japan).
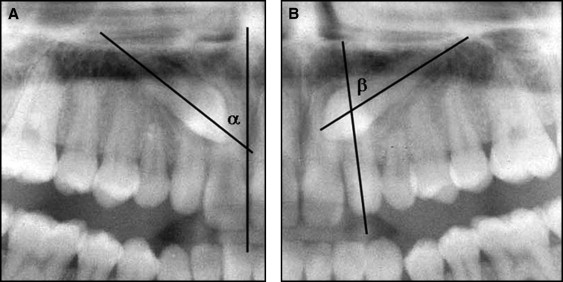
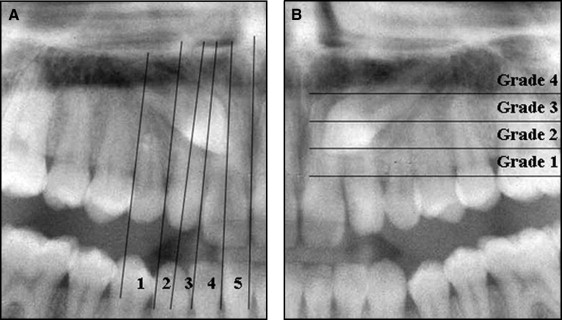
The following parameters related to the position of the impacted canine were recorded on orthopantomograms ( Figs 2 and 3 ): (1) inclination of the eruption path of the impacted canine to the midline (α) and to the long axis of the lateral incisor (β); (2) the medial position on the transverse plane of the impacted canine according to the projection of the tip of the crown in sectors (1 to 5); and (3) the vertical position of the canine crown relative to the adjacent maxillary incisor (grades 1 to 4).
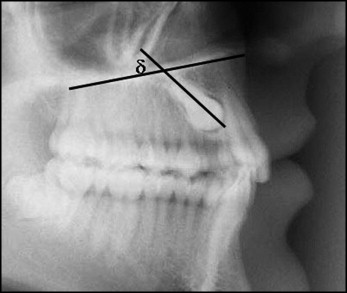
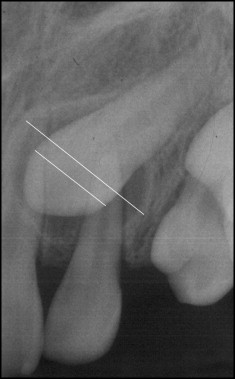
The sagittal inclination of the eruption path of impacted canine (δ), expressed by the angle between the axis of the impacted canine and the nasal line, was evaluated on the cephalograms ( Fig 4 ). Canine root development was categorized in 3 groups, by using intraoral x-rays and orthopantomograms (1, fully developed root; 2, open apex, but root longer than crown; 3, root shorter than crown). The relative width of the canine’s dental follicle was evaluated on intraoral radiographs. For that purpose, the ratio of the maximum width of the follicle to the width of the crown of the canine was estimated ( Fig 5 ).
Root length loss was assessed by using a method previously described by Mavragani et al. Crown and root lengths of the maxillary incisors were measured on the intraoral periapical films before and after active treatment. The measurements were made by using an image analysis system (NIS Elements Br; Nikon, Tokyo, Japan).
Any image distortion between the pretreatment and posttreatment radiographic exposures was corrected by using the crown length registrations, assuming that crown lengths were unchanged over the observation period. A correction factor was calculated to relate the pretreatment and posttreatment radiographs to each other. The apical root resorption per tooth in millimeters and in percentage of initial tooth length was calculated.
All radiographic measurements were performed by 1 examiner (E.M.G.B.) blinded concerning the origin of the x-rays. The reproducibility of the measurements was assessed by statistically analyzing the difference between double measurements taken at a 3-week interval. Double measurements were made for all maxillary incisors in 10 randomly selected patients. The systematic error was evaluated separately for crowns and roots, by using paired t tests between the double measurements. The measurement error, also separately for crowns and roots, was calculated by the formula: τ = SD/√2, where SD is the standard deviation of the differences between the double measurements.
No significant systematic errors were found, and the measurement errors were within acceptable limits (<1.000). Double measurements on 10 patients were also made regarding the characteristics of the impacted canines on orthopantomograms, lateral cephalometric radiographs, and intraoral radiographs, with acceptable results ( Table I ).
| n | Mean difference | SD | P | τ | |
|---|---|---|---|---|---|
| Crown | 40 | −0.11 | 0.199 | 0.292 | 0.141 |
| Roots | 40 | −0.30 | 0.511 | 0.168 | 0.361 |
| α angle | 10 | −0.01 | 0.797 | 0.969 | 0.564 |
| β angle | 9 | 0.46 | 1.295 | 0.322 | 0.916 |
| δ angle | 10 | 0.38 | 0.725 | 0.132 | 0.513 |
| Follicle/tooth ratio | 10 | 0.02 | 0.079 | 0.443 | 0.056 |
Statistical analysis
To test whether the recorded variables differed significantly between the 2 groups, the 2-sample t test was used for quantitative variables, and the chi-square test was used to compare the frequency distributions of the qualitative variables.
The 2-sample t test was performed to compare apical root resorption between the impaction and control groups for each tooth separately. For the comparison of root resorption between the impacted and nonimpacted sides in the impactiongroup, the paired t test was applied. This was done for both the central and lateral incisors. Root resorption of the maxillary incisors on the impacted side was compared with the mean value (between right and left sides) of apical resorption in the control group. The comparison was done with the 2-sample t test separately for the central and the lateral incisors.
Any association between pairs of variables, including root resorption values and the characteristics of the impacted canines, was evaluated by calculating the Spearman rank correlation coefficient. The level of significance was set at 5% ( P ≤0.05). All calculations were made with SPSS software for Windows (version 15.0; SPSS, Chicago, Ill).
Results
The 2 groups were well matched for all recorded variables. Mean values for root shortening of the maxillary incisors during treatment varied between 0.26 and 0.72 mm. Negative values, indicating root elongation, were observed among all incisors in both groups. The comparison of root resorption between patients with impacted canines and those with normally erupting canines showed no significant differences ( Table II ).
| Maxillary incisor | Impaction group | Control group | P | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | Minimum | Maximum | n | Mean | SD | Minimum | Maximum | ||
| Right lateral | 27 | 33 | |||||||||
| % | 3.01 | 9.24 | −17.82 | 19.24 | 3.27 | 16.24 | −80.82 | 23.73 | 0.940 | ||
| mm | 0.45 | 1.37 | − 2.85 | 3.08 | 0.72 | 1.66 | −6.60 | 4.01 | 0.493 | ||
| Right central | 31 | 33 | |||||||||
| % | 2.19 | 10.69 | −26.07 | 22.77 | 3.35 | 5.76 | −13.12 | 15.72 | 0.587 | ||
| mm | 0.43 | 1.71 | −3.65 | 4.47 | 0.56 | 0.91 | −1.70 | 2.80 | 0.689 | ||
| Left central | 31 | 33 | |||||||||
| % | 3.76 | 10.05 | −12.87 | 33.87 | 3.18 | 6.62 | −11.27 | 14.03 | 0.785 | ||
| mm | 0.63 | 1.67 | −1.68 | 6.68 | 0.54 | 1.03 | −1.49 | 2.27 | 0.795 | ||
| Left lateral | 30 | 30 | |||||||||
| % | 3.48 | 8.66 | −12.90 | 26.91 | 0.70 | 14.79 | −67.64 | 17.07 | 0.378 | ||
| mm | 0.49 | 1.25 | −2.05 | 3.41 | 0.26 | 1.59 | −5.83 | 2.63 | 0.538 | ||
No significant difference in apical root resorption was found between the impacted and nonimpacted sides for the central and lateral incisors ( Table III ). Similarly, the incisors on the impaction side showed no significant differences in root resorption compared with the incisors of the control group ( Table IV ).
| Impacted side (mm) | Nonimpacted side (mm) | P | |||||
|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | ||
| Lateral incisors | 26 | 0.33 | 1.53 | 26 | 0.56 | 1.02 | 0.512 |
| Central incisors | 31 | 0.48 | 1.96 | 31 | 0.58 | 1.37 | 0.800 |
| Impacted side | Controls (right-left) | P | |||||
|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | ||
| Lateral incisors | 29 | 0.44 | 1.54 | 28 | 0.51 | 1.61 | 0.871 |
| Central incisors | 31 | 0.48 | 1.96 | 31 | 0.54 | 0.79 | 0.878 |
The distributions of continuous and categorical variables related to the impacted canines are given in Table V . Angles α, β, and δ showed negative correlations with the severity of root resorption of the maxillary incisors ( Table VI ). The relationship was significant only for the maxillary left lateral incisor (α and β angles) and the maxillary right lateral incisor (δ-angle). Furthermore, the α and β angles were significantly correlated to the dental follicle/tooth ratio, with a significant correlation between them. The dental follicle/tooth ratio was not significantly correlated to root resorption of the maxillary incisors ( Table VI ).
| Categorical variables | Quantitative variables | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Categories | Frequency | Percent | Variable | Mean | SD | Minimum | Maximum |
| Medial position | 1 | 2 | 6.3 | α angle | 26.8 | 13.1 | 4.9 | 54.4 |
| 2 | 5 | 15.6 | β angle | 38.5 | 14.9 | 4.0 | 65.2 | |
| 3 | 11 | 34.4 | δ angle | 75.5 | 12.7 | 33.2 | 95.3 | |
| 4 | 9 | 28.1 | Follicle/tooth ratio | 1.51 | 0.24 | 1.2 | 2.0 | |
| 5 | 5 | 15.6 | ||||||
| Vertical position | 1 | 8 | 25.0 | |||||
| 2 | 17 | 53.1 | ||||||
| 3 | 7 | 21.9 | ||||||
| 4 | 0 | 0.0 | ||||||
| Root development | 1 | 10 | 31.3 | |||||
| 2 | 22 | 68.8 | ||||||
| 3 | 0 | 0.0 | ||||||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


