A Class III malocclusion associated with dental asymmetry is a complex diagnostic and treatment problem in orthodontics. The goals of maintaining or improving the facial profile and achieving good function are decisive factors when considering whether to plan a surgical or a nonsurgical treatment approach. A fixed appliance in combination with extractions could be considered for nonsurgical management of this type of malocclusion in the permanent dentition. This article presents the results of an orthodontic approach to a Class III subdivision malocclusion in an adult treated with mandibular first molar extractions. The extractions provided the space needed to correct the overjet and overbite and to improve the intercuspation.
Class III malocclusions represent a small proportion of all malocclusions among orthodontic patients. However, the treatment is a considerable clinical challenge because of the complex diagnosis and the difficult prognosis, mainly when the Class III relationship is associated with dental or skeletal asymmetries. There are 2 main treatment options for a Class III malocclusion that is identified after facial growth has been completed: orthodontic treatment and orthognathic surgery. For many patients with a Class III malocclusion, surgical treatment is the best alternative. The amount of the skeletal discrepancy usually determines whether a surgical correction is appropriate. However, in borderline cases, a balanced soft-tissue profile will help to determine whether patients are unsuitable for surgery. Generally, fixed appliances in conjunction with tooth extractions are considered the best option for nonsurgical management of adult Class III patients.
Traditionally, the extraction of the 4 premolars (mandibular first and mandibular second) is the most common choice. Alternative extractions have also been used. If the mandibular third molars are present, extraction of the mandibular first molars could be a good substitute option to solve the anteroposterior and vertical problems and obtain a Class I molar relationship. This approach is not indicated for all patients, because it requires first molar space closure, which is time-consuming. Also, the mandibular second molars have a tendency to tip mesially and lingually, requiring additional orthodontic mechanics to prevent that problem.
This case report describes a 20-year-old man with a Class III malocclusion. The treatment was carried out by using fixed appliances and mandibular first molar extractions. Our aim is to illustrate that, with careful case selection, a first molar extraction protocol can be relatively straightforward.
Etiology and diagnosis
This patient came to the orthodontic clinic at the Federal University of Rio de Janeiro in Brazil with the chief complaint of “dysfunctional bite.” Anamnesis was carried out, and the medical and dental histories showed nothing abnormal. The swallow and speech functions were normal, and the respiratory function was bucco-nasal. The extraoral assessment showed a straight profile, a slightly high mandibular plane angle, and an increased lower facial height. The nasolabial angle was slightly increased. No significant discrepancy between habitual occlusion and centric relation was found. The temporomandibular joints were normal, and his face was symmetric. Although he had a prominent lower lip, his facial appearance was pleasing, and he had no complaints about esthetics ( Fig 1 ).
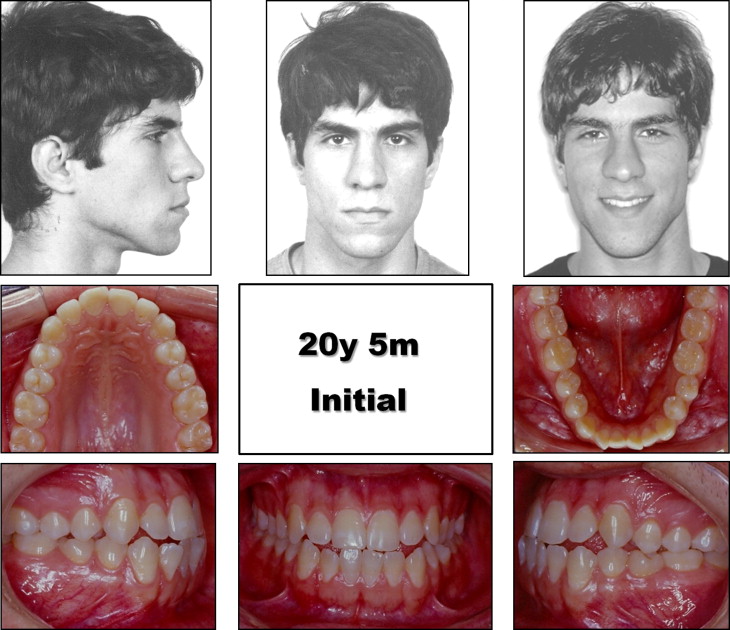
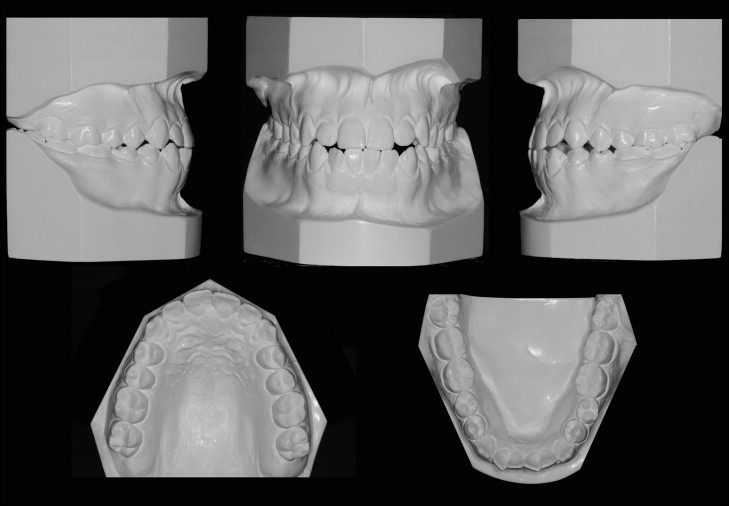
The intraoral examination showed a Class I molar relationship on the right side and a complete Class III molar relationship on the left side ( Fig 2 ). The maxillary and mandibular anterior teeth were in an edge-to-edge relationship, with no overjet or overbite. Crossbites of the maxillary left lateral incisor and first premolar were noted. The dental midline was not coincident with the facial midline. The maxillary midline was deviated 2 mm to the left. All permanent teeth were erupted, except for the maxillary third molars. Minor crowding was present only in the mandibular arch, with incisor irregularity of 1.2 mm. Significant rotations of the mandibular left second premolar and right second premolar were noted. The space analysis indicated a positive discrepancy of 1.3 mm in the mandibular arch. Both arches had a parabolic form.
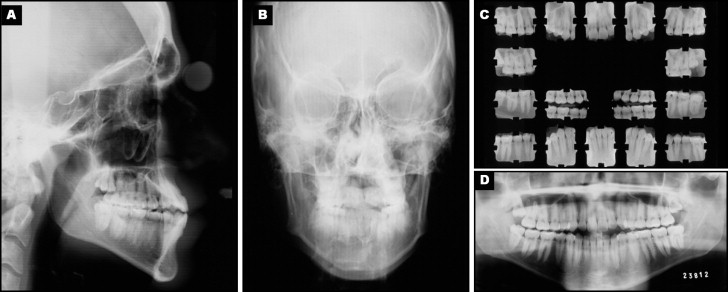
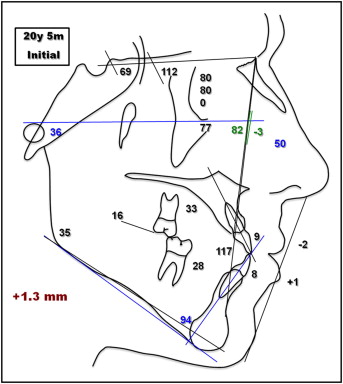
A panoramic radiograph confirmed the presence of all permanent teeth, including developing maxillary third molars ( Fig 3 ). A frontal radiograph showed no transverse or asymmetric skeletal problems. The lateral cephalometric evaluation ( Fig 4 ) indicated a skeletal Class I, bordering on mild skeletal Class III pattern (ANB, 0°). This skeletal pattern was confirmed by the Wits analysis that showed Wits appraisal (AO-BO) to be –4 mm. The mandibular planes were higher than normal limits, indicating a vertical growth pattern (SN.GoGn, 35°; FMA, 36°; SN.y-axis, 69°). The maxillary and mandibular incisors were protruded (1.NA, 33°; 1.NB, 28°) and proclined (1-NA, 9 mm; 1-NA, 8 mm). The lower facial profile was straight, with the upper lip lying behind the S line, and the lower lip passing it slightly (S-LS, –2 mm; S-LI, 1 mm).
Treatment alternatives
Orthognathic surgery was not a viable treatment option because the skeletal deficiency was not clinically significant and the patient was satisfied with his facial profile and appearance. Maximum anchorage was discussed for en-masse movement of the mandibular teeth and correction of the maxillary dental asymmetries, but the patient refused to use any kind of temporary anchorage device. Maxillary second premolar and mandibular first premolar extractions could be a treatment option; however, no changes in the upper lip were desirable. Because the mandibular third molars were in an ideal position and the patient was cooperative, we chose to extract the mandibular first molars.
Treatment alternatives
Orthognathic surgery was not a viable treatment option because the skeletal deficiency was not clinically significant and the patient was satisfied with his facial profile and appearance. Maximum anchorage was discussed for en-masse movement of the mandibular teeth and correction of the maxillary dental asymmetries, but the patient refused to use any kind of temporary anchorage device. Maxillary second premolar and mandibular first premolar extractions could be a treatment option; however, no changes in the upper lip were desirable. Because the mandibular third molars were in an ideal position and the patient was cooperative, we chose to extract the mandibular first molars.
Treatment objectives
The treatment objectives were to maintain the patient’s profile, improve dental and smile esthetics, level and align the maxillary and mandibular dental arches, correct the dental asymmetries, achieve Class I molar and canine relationships on both sides, achieve normal overjet and overbite, and establish a good functional occlusion.
To achieve all the desired objectives, we decided to use fixed orthodontic appliances with extraction of the mandibular first molars to align and level, correct the overbite and overjet, and achieve a Class I relationship. The maxillary third molars would also be extracted to facilitate distalization of the maxillary right posterior teeth to correct the dental asymmetries (midline).
Treatment progress
The molars were banded, and the remaining teeth were bonded with a standard edgewise fixed appliance (0.022 × 0.028 in; Morelli, São Paulo, Brazil) ( Fig 5 ). The teeth were aligned and leveled by using a sequence of round steel continuous archwires of 0.014- to 0.020-in stainless steel. Subsequently, rectangular steel archwires of 0.018 × 0.025-in stainless steel were used and were followed by 0.019 × 0.026-in rounded-edge stainless steel working wires to allow final space closure and occlusal adjustment. All the steel archwires were conformed according to the patient’s initial arch form. Elastic chains were used to move the second molars mesially, with anchorage reinforcement on the mandibular teeth (right second premolar to left second premolar). Lingual buttons were used to control the rotation of the premolars and the second molars during space closure. Class II intermaxillary elastics and sliding jigs were used on the right side to distalize the teeth and correct the maxillary midline. The right third molar was extracted before this phase to facilitate the distalization. Class III and Class II elastics were used to coordinate the arches; after a good occlusal relationship was obtained, detailing and finishing procedures were undertaken.


