Protraction of posterior teeth into edentulous spaces is a challenge. This report describes the treatment of a 19-year-old woman with missing mandibular first molars owing to caries. A fixed functional appliance was used for anchorage reinforcement during mandibular second molar protraction. Eight millimeters of bilateral protraction was done with bodily mesial movement of the molars and no lingual tipping of the incisors.
Highlights
- •
Anchorage reinforcement during second molar protraction was provided using a fixed functional appliance.
- •
No skeletal or dental Class II correction was attempted using the fixed functional appliance.
- •
Use of stiff archwires prevented tipping of second molars during molar protraction phase.
Effective space management of missing posterior teeth is a great challenge in orthodontic treatment. Edentulous posterior sites are commonly seen in an adult population. The most commonly observed missing teeth are first molars, often owing to caries, and second premolars, which are the most common congenitally missing teeth. The sequel of missing mandibular first molars is usually tipping and drifting of adjacent teeth, supraeruption of unopposed teeth, poor interproximal contacts, poor gingival contours, reduced interradicular bone, and pseudopockets.
Treatment options for missing posterior teeth commonly include fixed prosthodontic bridges or endosseous implants. Although both are viable treatment options, the use of fixed partial dentures may compromise the longevity of adjacent prepared teeth with the risk of secondary caries and mechanical failures, whereas endosseous implants can increase the financial burden for patients. Orthodontic space closure of edentulous sites is an alternative treatment option. However, attempts at space closure by protraction of posterior teeth into the edentulous sites without anchorage reinforcement bears the risk of anchorage loss, thereby leading to a compromised occlusion. Historically, extraoral appliances such as chincup and facemask have been used for protraction of posterior teeth. However, use of extraoral devices depends on patient compliance, and it has been reported that patient compliance is generally overestimated when similar devices are used for orthopedic purposes. Hemisection of deciduous teeth has also been advocated to encourage more mesial eruption of the permanent teeth into the missing-tooth regions. Recently, there have been case reports in the literature on the use of mini-implants for protraction of mandibular posterior teeth into edentulous sites. However, mini-implants placed in interradicular regions can cause root damage because of improper placement of the devices, which can subsequently lead to implant failure.
Thus, development of alternative methods capable of providing absolute anchorage while protracting posterior teeth into edentulous sites is desirable. Fixed functional appliances have traditionally been used for Class II correction. The use of such appliances results in a combination of mild skeletal effects along with dentoalveolar changes such as retroclination of the maxillary incisors and proclination of the mandibular incisors, and distalization of the maxillary molars and mesial movement of the mandibular molars. The aim of this report was to use a fixed functional appliance for anchorage reinforcement during space closure by protraction of the posterior teeth into the edentulous spaces without Class II correction.
Diagnosis and etiology
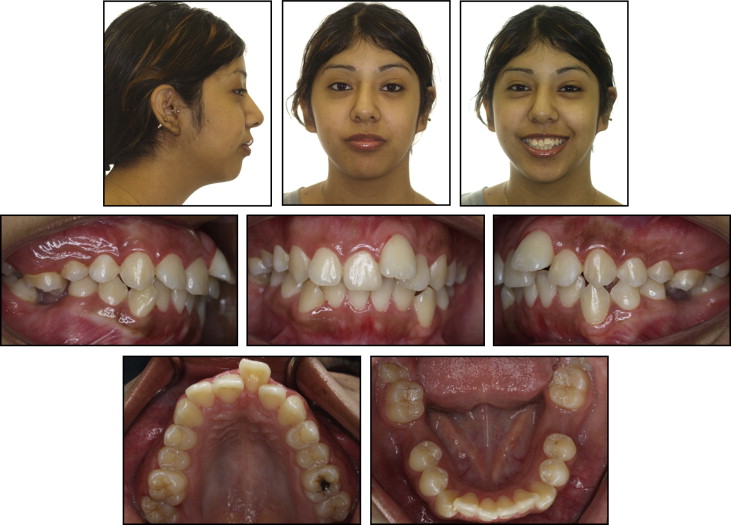
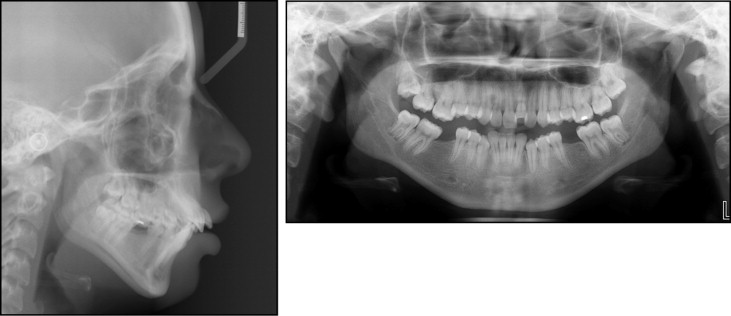
A 19-year-old woman came to the orthodontic department at University of Connecticut Health Center with a chief complaint of “crooked teeth.” Her previous medical history was not significant, and no history of habits was reported. Her dental history showed that the mandibular left and right first molars were extracted because of caries approximately 4 years previously. She had a Class II malocclusion on an underlying Class II skeletal base with a normal sized maxilla, a short mandible, and a vertical growth pattern ( Fig 1 , Table ). Dentally, the patient had proclined and forwardly placed maxillary incisors and normally inclined and forwardly placed mandibular incisors with U-shaped maxillary and mandibular dental arches, missing mandibular right and left first molars with 8 mm of extraction space bilaterally, mesially tipped mandibular second molars bilaterally ( Fig 2 ), extruded maxillary left and right first molars, an end-on canine relationship, moderate crowding in both arches, an increased overjet, a 4-mm overbite, and a 3-mm curve of Spee in the mandibular arch. Facially, the patient had a leptoprosopic facial type with a convex soft tissue profile, a right angled nasolabial angle, and 100% maxillary incisor and 70% mandibular incisor display on smiling. The mandibular midline was coincident with the facial midline, and the maxillary midline was shifted 2 mm to the left, along with incompetent lips ( Fig 2 ) and lip strain on closure.
| Pretreatment | Posttreatment | |
|---|---|---|
| SNA (°) | 77 | 77 |
| SNB (°) | 71 | 71 |
| ANB (°) | 6 | 6 |
| SN-GoGn (°) | 47 | 48 |
| FMA (°) | 41 | 42 |
| U1-SN (°) | 118 | 92 |
| U1-NA (°) | 42 | 19 |
| U1-NA (mm) | 12 | 3 |
| IMPA (°) | 90 | 92 |
| L1-NB (°) | 35 | 33 |
| U1-NB (mm) | 13 | 11 |
| E-line–upper lip (mm) | 1 | −5 |
| E-line–lower lip (mm) | 5 | −2 |
Treatment objectives
The treatment objectives for this patient were to (1) improve the soft tissue profile and relieve the lip incompetence with minimal changes to the skeletal vertical dimensions, (2) manage the space of the missing mandibular first molars by protraction of the mandibular second molars into the first molar regions bilaterally, (3) achieve simulated Class II molar and Class I canine relationships by retraction of the maxillary incisors and protraction of the mandibular molars, (4) relieve the crowding in both arches, and (5) reduce the increased overjet.
Treatment objectives
The treatment objectives for this patient were to (1) improve the soft tissue profile and relieve the lip incompetence with minimal changes to the skeletal vertical dimensions, (2) manage the space of the missing mandibular first molars by protraction of the mandibular second molars into the first molar regions bilaterally, (3) achieve simulated Class II molar and Class I canine relationships by retraction of the maxillary incisors and protraction of the mandibular molars, (4) relieve the crowding in both arches, and (5) reduce the increased overjet.
Treatment alternatives
The alternative treatment plans that were considered entailed extraction of only the maxillary premolars with retraction of the incisors and endosseous implants, or fixed partial dentures placed for the missing mandibular first molars. Implants would increase the overall treatment cost for the patient, and she was unwilling to undergo this procedure. In addition, the use of fixed partial dentures could compromise the longevity of the prepared adjacent teeth in the long term. The use of mini-implants or miniplates for protraction of the posterior teeth into the edentulous sites could have been considered as a treatment alternative.
Treatment progress
Treatment was initiated by bonding all teeth with a 0.022-in slot MBT (McLaughlin, Bennett, and Trevisi) prescription, which had 6° of lingual crown torque on the mandibular anterior brackets. In the mandibular arch, initial leveling and alignment was done with 0.16-in nickel-titanium archwires from the left second premolar to the right second premolar without engaging the tipped second molars. The archwire was gradually increased to 0.021 × 0.025-in stainless steel. An uprighting spring was fabricated and placed on the tipped second molars to upright them ( Fig 3 , A ). A seating elastic was used in the anterior segment to prevent the bite from opening during uprighting of the tipped molar. The mechanics involved in using the uprighting spring are shown more in Figure 3 , B . An uprighting spring is a 1-couple system. An intrusive component of force exists in the anterior segment along with an extrusive force on the molar with a counterclockwise moment (moment of couple) to upright the tipped molar. In addition, the point of force application on the molar (buccal tube) is usually ahead of the center of resistance of the molar, thereby leading to an additional moment (moment of force) in the counterclockwise direction that can further help in uprighting the tipped molar.
In the maxillary arch, the patient was referred for extraction of the maxillary first premolars. Initial leveling and alignment were performed in the maxillary arch using a 0.016-in nickel-titanium archwire. The archwires were progressively increased to 0.021 × 0.025-in nickel-titanium. Space closure was performed using loop mechanics; a 0.019 × 0.025-in T-loop archwire was fabricated for en-masse retraction of the maxillary anterior teeth ( Fig 4 , A ). After space closure, the archwire was increased to a stiff 0.021 × 0.25-in steel archwire with the wire cinched distal to the molars to prevent any spaces from opening up and to create the maxillary arch as a single unit.


