Apart from a few exceptions, dental practitioners are not familiar with sectional images (as those provided by cone beam computed tomography [CBCT]). In addition, the maxillofacial region is a complex area from an anatomic point of view including structures of peculiar shape; this may add to that complexity of their appearance in CBCT. As a result, a thorough knowledge of the tomographic anatomy of the maxillofacial region was necessary. This chapter reviews pertinent anatomical structures of the maxillofacial region in the axial, coronal, sagittal planes, as well as custom planes. Related pathology is also shown and discussed.
Key points
- •
Multiplanar imaging-reformatting (MPR) has significantly increased the diagnostic accuracy and efficiency of the knowledgeable dental professional.
- •
Reviewing the dental and maxillo-facial structures in all perspectives may reveal hidden aspects of relevant disease and may enhance diagnosis.
- •
The novelty of the diagnostic tool (CBCT) and the unfamiliarity of the generated sectional images make knowledge of the anatomy mandatory.
- •
Major anatomical structures, commonly seen in CBCT routine scans are reviewed as well as related pathology, including the para-nasal sinuses, neck and cervical spine, skull base and more.
Introduction
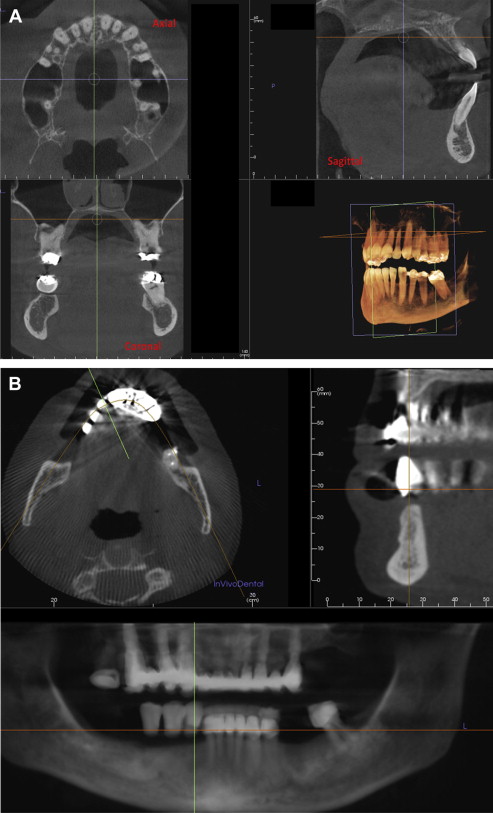
Multiplanar imaging has offered an unparalleled diagnostic approach when dealing with an unknown entity (pathologic or not) that has stood as a diagnostic challenge. This concept is inherent to volumetric type of data (computed tomography [CT], cone beam computed tomography [CBCT], magnetic resonance imaging) and has offered the diagnostician the unique ability to generate images (sections) at different planes (flat or curved). Because a volume of data has been acquired and stored by CBCT, this data can be reformatted or realigned and several different types of images can be synthesized in any way the diagnostician requires, thus eliminating the superimposition of the area or entity under investigation with other neighboring structures and allowing its assessment from all perspectives. With multiplanar imaging, the diagnostician/operator can re-create images in different planes (flat or curved) with very simple functions, increasing the diagnostic efficiency in the hands of the knowledgeable individual in an unparalleled way ( Fig. 1 ).
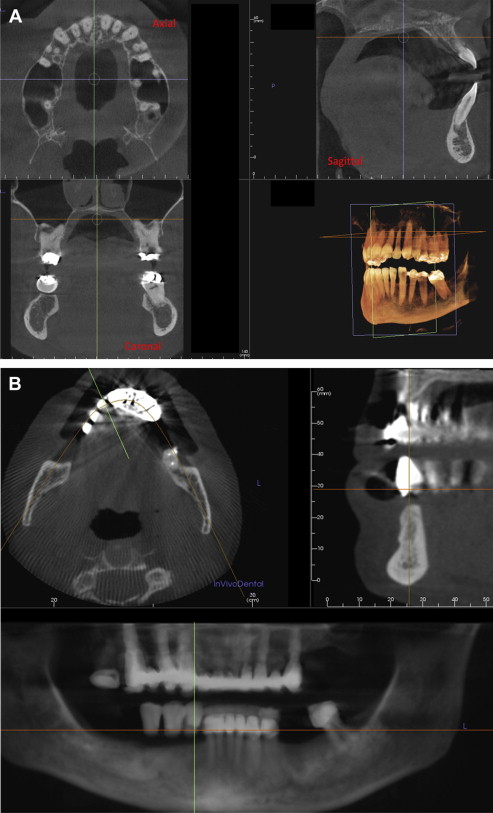
Undoubtedly, multiplanar imaging, as provided by cone-beam imaging, is a novelty for the dental professional: most dentists and specialists, with only a few exceptions, are not familiar with diagnostic imaging in different planes, although they are keen on interpreting projectional images as those produced by traditional dental imaging modalities (intraoral radiography and panoramic radiography). Sectional images (tomographic images) reveal the spatial relationship of the various known anatomic structures in the maxillofacial region, which was more or less lost in projectional imaging.
In this article the appearance of several anatomic structures of the maxillofacial region as well as the head and neck region in general is reviewed; these structures are analyzed in all 3 basic tomographic planes (axial, coronal, sagittal). Additional reconstructed images may be used to view certain anatomic areas from all aspects. To review the anatomy of the maxillofacial region in a systematic way, the maxillofacial region is divided into smaller areas of interest. Emphasis in this topographic anatomic review is placed on areas that may demonstrate a higher incidence of occult disease. Emphasis is also on structures outside the dentoalveolar region. The anatomy of dental and dentoalveolar structures has been thoroughly reviewed elsewhere.
Introduction
Multiplanar imaging has offered an unparalleled diagnostic approach when dealing with an unknown entity (pathologic or not) that has stood as a diagnostic challenge. This concept is inherent to volumetric type of data (computed tomography [CT], cone beam computed tomography [CBCT], magnetic resonance imaging) and has offered the diagnostician the unique ability to generate images (sections) at different planes (flat or curved). Because a volume of data has been acquired and stored by CBCT, this data can be reformatted or realigned and several different types of images can be synthesized in any way the diagnostician requires, thus eliminating the superimposition of the area or entity under investigation with other neighboring structures and allowing its assessment from all perspectives. With multiplanar imaging, the diagnostician/operator can re-create images in different planes (flat or curved) with very simple functions, increasing the diagnostic efficiency in the hands of the knowledgeable individual in an unparalleled way ( Fig. 1 ).
Undoubtedly, multiplanar imaging, as provided by cone-beam imaging, is a novelty for the dental professional: most dentists and specialists, with only a few exceptions, are not familiar with diagnostic imaging in different planes, although they are keen on interpreting projectional images as those produced by traditional dental imaging modalities (intraoral radiography and panoramic radiography). Sectional images (tomographic images) reveal the spatial relationship of the various known anatomic structures in the maxillofacial region, which was more or less lost in projectional imaging.
In this article the appearance of several anatomic structures of the maxillofacial region as well as the head and neck region in general is reviewed; these structures are analyzed in all 3 basic tomographic planes (axial, coronal, sagittal). Additional reconstructed images may be used to view certain anatomic areas from all aspects. To review the anatomy of the maxillofacial region in a systematic way, the maxillofacial region is divided into smaller areas of interest. Emphasis in this topographic anatomic review is placed on areas that may demonstrate a higher incidence of occult disease. Emphasis is also on structures outside the dentoalveolar region. The anatomy of dental and dentoalveolar structures has been thoroughly reviewed elsewhere.
Nose and paranasal sinuses
The paranasal sinuses are 4 pairs of air-filled osseous cavities that surround the nose and the orbits and that belong to the maxillary (maxillary sinuses), ethmoid (ethmoid air cells), frontal (frontal sinuses), and sphenoid (sphenoid sinuses) bones, respectively.
Paranasal sinuses are best assessed in coronal sections; in fact, coronal images are the most appropriate for the evaluation of anatomic structures that have a posteroanterior orientation. The maxillary, ethmoid, and sphenoid sinuses as well as the nasal cavity and certain structures in the skull base will be optimally imaged in these views. In this review, the anatomic structures of interest ventrally to dorsally (or anterior to posterior) are reviewed (see Figs. 21–26 ).
At the level of maxillary premolars, the coronal images section through the frontal sinuses, the orbits, the anterior aspect of the maxillary sinuses, the ethmoid air cells, and the nasal cavity. The various anatomic structures of interest are addressed by means of importance to the dental professional (anatomic proximity to dental structures).
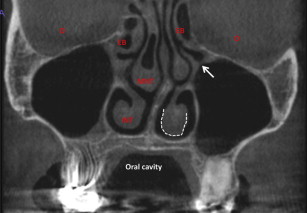
The nasal cavity is seen as a pyramidal-shaped air cavity that is divided in 2 distinct, fairly symmetric, noncommunicating air cavities by the nasal septum. Each one of them is separated further into smaller, blind (open) chambers by 3 elongated or arch-shaped osseous projections that originate from its lateral walls: these are the inferior, middle, and superior nasal conchae or turbinates, which border the inferior, middle, and superior nasal meatuses (chambers) ( Fig. 2 ). Only the inferior concha is an independent facial bone; the rest are parts of the ethmoid bone. Although they are lined by 2 to 3 mm of mucosa, there are identifiable air passageways that guide the inhaled air to the paranasal sinuses. Shape alterations of the nasal chambers and the septum may affect the flow of air through the nose and may be associated with upper airway obstructive phenomena (ie, sleep apnea). In fact, a deviated nasal septum is a common cause of sleep apnea (see Fig. 2 ). The nasal turbinates may sometimes be pneumatized; in this case, instead of a dense bony process, the nasal turbinate is presented as an extension of the ethmoid air cells, filled with air, and surrounded by a thin corticated border. This phenomenon is considered an anatomic variant, and the pneumatized turbinate is best known as “concha bullosa,” and is more frequently seen in the middle nasal turbinates; its incidence ranges between 15% and 45%. Conchae bullosa may be inflamed because they are communicating with the ethmoid air cells; however, their presence does not seem to affect the pathogenesis of sinus inflammation (sinusitis). Sometimes, conchae bullosa may contribute to upper airway obstruction because they may obliterate the air passageways in the nasal cavity (see Fig. 2 ).
Another prominent osseous canal is identified in the coronal sections through the anterior third of the nasal cavity: the nasolacrimal duct, which originates at the floor/medial wall of the orbit, opens into the inferior nasal meatus ( Fig. 3 ), and drains tears form the orbit into the inferior meatus.
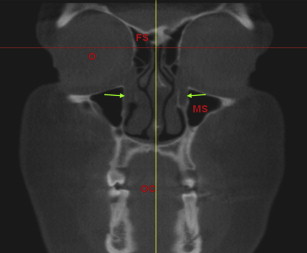
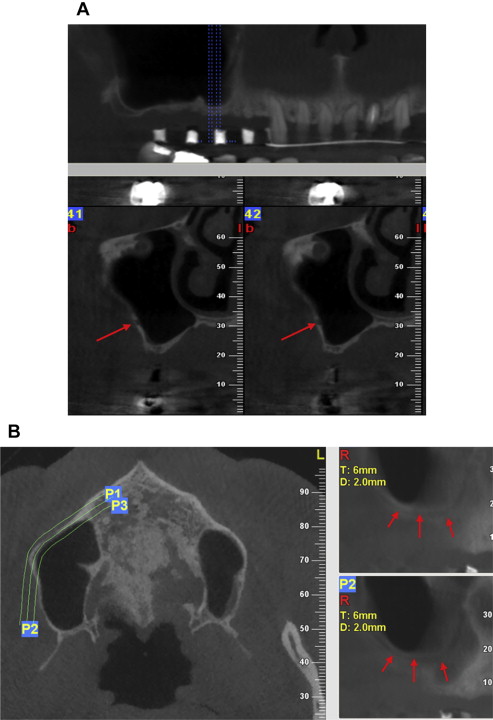
The maxillary sinuses are the largest among the various paranasal sinuses ( Figs. 4–6 ). These air cavities belong to the maxillary bone. As all air cavities will be displayed as uniform dark or black because air is depicted as a very low density structure in computed tomography (CT or CBCT). The presence of any other appearance than black may represent pathologic abnormality in the air cavity. Almost pyramidal in shape, with the base of the pyramid being the medial wall or the wall that is shared with the nasal cavity and the tip of the pyramid being the zygomatic process of the maxilla (anterior end of the zygomatic arch). The other sides of the pyramid are the superior wall (roof of the maxillary sinus), which is shared with the orbit, the lateral wall, the anterior wall, and the posterior wall. CBCT images may provide a detailed evaluation of the integrity of the walls of the maxillary sinuses as well as the presence of disease in the air cavities. The posterior superior alveolar neurovascular canals may be sometimes be seen on the lateral wall of the maxillary sinus as a small, pinhead-size, low-density areas (in coronal images) running almost parallel to the floor of the sinus and turning cephalad (superior) in the premolar region (in panoramic reconstructions). Its diameter, as with all vascular canals, may provide information as far as it concerns its bleeding potential if injured during sinus grafting procedures (see Fig. 4 ).
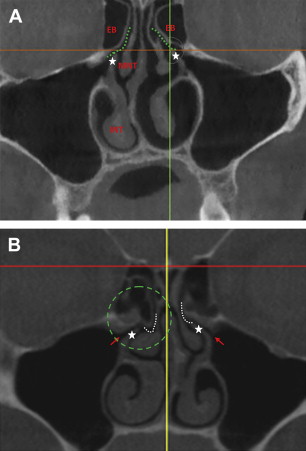
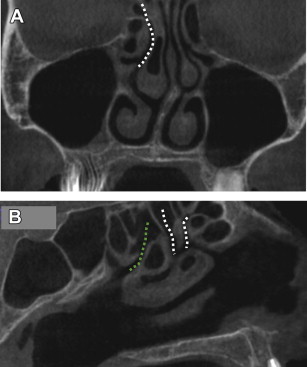
The draining sites of the maxillary sinuses (maxillary sinuses’ ostia) are likely to be visualized in coronal images toward the anterior third of the sinus cavities (from front to back) and may not be both identifiable in the same coronal plane. The ostium of the maxillary sinus is a small opening in the medial wall of the maxillary sinus (or lateral wall of the nasal cavity) toward the superior aspect, leading into the ethmoid infundibulum, a narrow passageway that opens into the middle nasal meatus; it is formed partially by the ethmoid bone (ethmoid bulla-superior) and a thin pointy osseous process on the lateral wall of the nasal cavity known as the uncinate process. The maxillary sinus and the anterior ethmoid air cells drain into the middle nasal meatus through the infundibulum. The maxillary sinus ostium and the infundibulum are parts of the ostiomeatal complex, a broader anatomic unit that serves as the draining site of the maxillary, anterior ethmoid, and frontal sinuses. Slightly higher, in the same sections, the draining path of the frontal sinus is identified; this is known as the frontal recess. The narrow arch-shaped passageway between the ethmoid bulla and the middle turbinate just superior to the infundibulum is the hiatus semilunaris, named so because of its curved, almost semilunar shape, in the sagittal views (see Fig. 5 ). This hiatus semilunaris connects the ethmoid infundibulum to the frontal recess. The semilunar hiatus is the final segment of the drainage pathway from the maxillary sinus and ethmoidal infundibulum to the middle meatus. The narrow and delicate nature of the above-mentioned draining sites makes them vulnerable to possible blockage when inflammation occurs in their vicinity. Moreover, their close proximity to each other renders them possible paths for spread of infection. Identification of the draining sites and assessment of their integrity is important in patients who will undergo maxillary sinus grafting procedures. Blockage of the draining site may prevent the aeration of the sinus cavity and result in accumulation of inflammatory products into the sinus (see Fig. 6 ). This fine and delicate anatomy of the ostiomeatal complex may be grossly altered if sinus surgery has occurred ( Fig. 7 ).

The ethmoid air cells or sinuses are numerous, small, mostly square, air cavities that are separated by thin bony walls, grouped in 2 orthogonal prisms located on either side of the superior nasal cavities, and run parallel to the nasal cavities through their entire length (from front to back). They are bordered from the orbits with the lamina papyracea, a paper-thin osseous wall, and from the nasal cavities with the superior and middle nasal turbinates ( Fig. 8 ). The anterior and middle ethmoid air cells drain into the middle nasal meatus, whereas the posterior ethmoid air cells drain into the superior nasal meatus ( Fig. 9 ).
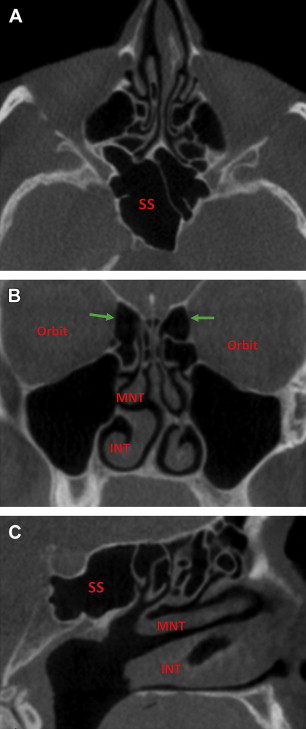
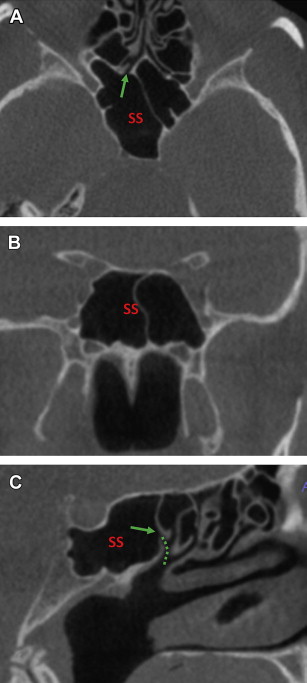
The sphenoid sinuses are the posterior-most air cavities and belong to the sphenoid bone. Their shape is similar to that of a truncated pyramid with its base being the bony roof of the nasopharynx; its roof, the sella turcica (pituitary fossa), and its lateral walls border the cavernus sinuses on either side of the body of the sphenoid bone. The sphenoid sinuses drain to the superior nasal meatus through a small opening in their anterior wall, the spheno-ethmoidal recess ( Fig. 10 ).
Important anatomic entities, such as the optic canal, the foramen rotundum, and the vidian canal, are closely related to the sphenoid sinuses and will be addressed in later discussion in the anatomic review of the skull base (see Figs. 25 and 26 ).
The frontal sinuses are 2 funnel-shaped air cavities identified superior to the ethmoid air cells and the nasal cavities and belong to the frontal bone. They demonstrate a great deal of variation in shape and size. A septum, which is frequently deviated, separates the right from the left and asymmetry between the 2 is not uncommon. They drain into the middle nasal meatus through the frontal recess, a thin passageway, part of the ostio-meatal complex (discussed earlier).
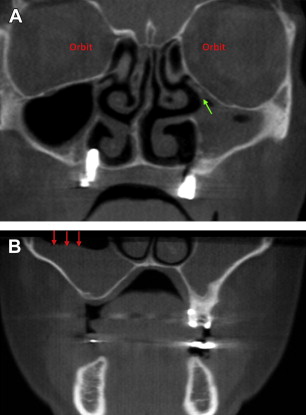
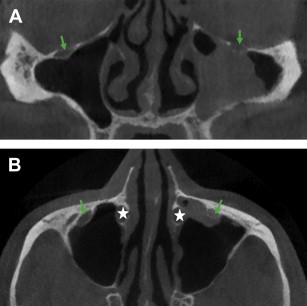
The orbits are visualized toward the anterior third of the face as well as the ethmoid air cells, the most anterior part of which is sectioned at this level. These views are excellent for the assessment of the integrity of the osseous walls of the orbits and their borders. A short osseous canal seen originating from the floor of the orbit and directed inferomedially to the anterior wall of the maxillary sinus is the infraorbital foramen, which accommodates the infraorbital nerve ( Fig. 11 ). Lamina papyracea, a paper-thin osseous diaphragm that belongs to the ethmoid bone and serves as the medial orbital wall, stands as the boundary between the orbit and the ethmoid air cells (see Figs. 6 A and 8 B).
Unfortunately, the soft tissue contrast of CBCT is inadequate for the assessment of the orbital content (eye globe, fat, and musculature of the eye globe).
Inflammation is by far the most common pathologic entity among the ones affecting the paranasal sinuses. Moreover, it seems that it is a frequent occult pathologic entity in CBCT scans prescribed for other diagnostic concerns.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


