Introduction
Although rapid maxillary expansion has been extensively studied in noncleft patients, scarce evidence of maxillary effects is found for patients with oral clefts. Our objective was to evaluate the dentoalveolar effects of rapid maxillary expansion in children with unilateral complete cleft lip and palate compared with noncleft patients.
Methods
The experimental group included 25 patients with unilateral complete cleft lip and palate and posterior crossbite (9 girls, 16 boys; mean age, 10.6 years). The control group comprised 27 noncleft patients with posterior crossbite (14 boys, 13 girls; mean age, 9.1 years). The experimental group had lip and palate repairs at 3 and 12 months of age, respectively, and maxillary expansion was indicated before a secondary alveolar bone graft. Digital dental models were obtained immediately before expansion and 6 months after expansion with a laser scanner. Canine and posterior tooth inclinations, transversal widths, arch perimeters, arch lengths, palatal depths, and palatal volumes were digitally measured. The paired t test was used for interphase comparisons, and the independent t test was used for intergroup comparisons ( P <0.05).
Results
In the experimental group, expansion produced buccal tipping of the canines and posterior teeth and significant increases of all maxillary transverse measurements, arch perimeter, palatal volumes, and palatal depths; only arch lengths decreased. No differences were observed between the groups for any measurement, except for intermolar distance.
Conclusions
Rapid maxillary expansion produced similar changes in the patients with unilateral complete cleft lip and palate compared with the noncleft patients except for arch length and palatal depth that decreased after expansion in the children with oral clefts.
Highlights
- •
Dentoalveolar effect of hyrax rapid maxillary expansion (RME) was studied in children with cleft lip and palate.
- •
Maxillary arch width, arch perimeter, and palatal volume increased in the unilateral complete cleft lip and palate (UCLP) group.
- •
Arch length decreased in the UCLP group.
- •
Canine and posterior teeth tipped buccally in the UCLP group.
- •
Dentoalveolar effects of RME were similar in children with and without UCLP.
Unilateral complete cleft lip and palate (UCLP) is the most frequent type of nonsyndromic oral cleft. The rehabilitation process of these patients is challenging and chronologically extensive. Lip and palate repair are performed at early stages of life. The operated lip and palate influence maxillary growth, causing anteroposterior, vertical, and transversal maxillary deficiencies. Maxillary arch constriction is frequently observed in operated patients with UCLP. Athanasiou et al stated that the frequencies of crossbite in children with UCLP in the deciduous, mixed, and permanent dentitions vary from 45.8% to 61.1%. When evaluating the Oslo CLP Growth file, Semb found that approximately 25% of the patients had crossbite. Pruzansky and Aduss, evaluating 33 children with UCLP during the deciduous dentition, noticed that only 30% of the crossbites were related to collapse of the arch. A recent study showed that children with UCLP in the mixed dentition tended to have more severe maxillary transverse constrictions because the maxilla is more retrognathic.
In the rehabilitation protocol for patients with UCLP, maxillary expansion is frequently necessary before the secondary alveolar bone graft procedure. Rapid maxillary expansion (RME) is commonly used for correcting the maxillary constriction. RME increases the maxillary dental arch, aligns the maxillary segments, and provides space in the alveolar cleft for a bone graft. The skeletal and dental effects of RME in patients with UCLP have been assessed previously in clinical experiments and finite element studies. Asymmetric expansions were found by several authors. Isaacson and Murphy reported no correlation between the cleft location and the relative amount of lateral movement of each maxillary segment, emphasizing that RME laterally repositioned the maxillary segments in an unpredictable manner. Pan et al, Holberg et al, and Gautam et al considered that the amount of displacement at the cleft side was greater than that at the noncleft side, and the amount of posterior expansion was greater than the anterior expansion.
Evaluating dental models, Isaacson and Murphy showed that the anterior and posterior teeth in each buccal segment expanded laterally by approximately the same amount that the expansion screw was opened. The amount at the gingival level, however, was often not as great, suggesting lateral tipping of the teeth, without differences for the cleft and noncleft segments. Pan et al, Gautam et al, and Tindlund et al concluded that a marked amount of displacement and deformation occurs in the dental region on both cleft and noncleft sides. According to these authors, the most significant transverse displacement was found at the crown of the maxillary permanent first molar, with a decreasing effect toward the anterior region of the dental arch. Wang et al observed that the reaction force at the molar on the noncleft side was greater than at the cleft side because expansion met more resistance on the noncleft side. Façanha et al found similar changes in dental models when comparing Haas-type and hyrax expanders in UCLP patients. They found that RME in UCLP patients produced significant increases of maxillary transversal widths without differences between the appliances. Maxillary expansion occurred in a pyramid shape, with the base located at the oral side, increasing the cleft area according to clinical and finite element model studies.
No previous studies of RME in cleft patients have analyzed arch volumes and tooth inclinations. Additionally, no previous studies have compared the RME effects in cleft and noncleft patients. Therefore, the aim of this study was to evaluate the dentoalveolar effects of RME in children with UCLP compared with noncleft patients. The null hypothesis was that RME produces similar effects in patients with and without oral clefts.
Material and methods
This clinical prospective study was approved by the ethical committee (number 164.747) at the Hospital for Rehabilitation of Craniofacial Anomalies (USP/Bauru–Brazil). Children, parents, or guardians signed informed consents.
The sample size calculation showed that to detect a minimum difference of 0.5 mm in maxillary width measurements, with a standard deviation of 0.8 mm at a significance level of 5% and power of 80%, it was necessary to have a minimum of 19 subjects in each group.
Therefore, the experimental group consisted of 25 patients with UCLP (9 girls, 16 boys) with a mean age of 10.6 years. This group was consecutively selected from February 2010 to March 2011 at the Orthodontic department of Hospital for Rehabilitation of Craniofacial Anomalies. The inclusion criteria were (1) both sexes, (2) mixed dentition or early permanent dentition with no missing posterior teeth, (3) lip and palatal repair in early childhood, (4) maxillary constriction and need for maxillary expansion before the secondary alveolar bone graft, (5) no previous bone graft surgery, and (6) enough initial palatal depth to receive the Haas-type expander. Patients with a shallow palate were expanded with hyrax appliances and were not selected for this study.
The control group comprised 27 children without cleft lip and palate (14 boys, 13 girls) with a mean age of 9.1 years, treated at the orthodontic clinic of Interceptive Orthodontics Course from PROFIS/Bauru, Brazil. This group was consecutively selected from February 2012 to February 2014. The inclusion criteria were (1) both sexes, (2) mixed dentition or early permanent dentition with no missing posterior teeth, (3) maxillary constriction and need for maxillary expansion, and (4) maxillary expansion performed with a Haas-type appliance.
The exclusion criteria for both groups were (1) need for maxillary protraction, (2) associated syndromes, and (3) previous orthodontic intervention.
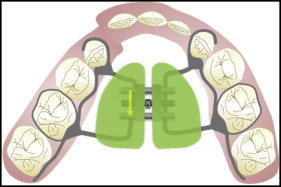
Patients in the experimental group had lip and palate repairs at 3 and 12 months of age, respectively. Maxillary expansion was performed before the secondary alveolar bone graft procedure. RME was carried out with Haas-type expanders in all patients in both groups. The expander had circumferential clasps bonded on the canines and bands on the deciduous second molars. A lingual bar extended to the permanent first molars ( Fig 1 ). All patients underwent the same activation protocol of 1 complete turn a day (2/4 screw activation in the morning and 2/4 screw activation in the evening) for 7 days regardless of the anteroposterior arch relationship. When necessary, more activation was performed until a slight overcorrection was reached with the palatal cusps of the maxillary first molars in contact with the buccal cusps of the mandibular first molars. After the active expansion phase, the appliance was maintained as retention for 6 months.
Dental models were obtained before expansion and 6 months postexpansion, at appliance removal. The dental models with standard trimming were scanned with a laser scanner (R700 3D; 3Shape A/S, Copenhagen, Denmark). The images were saved in STL format, compatible with Windows and other specific software of tridimensional images.
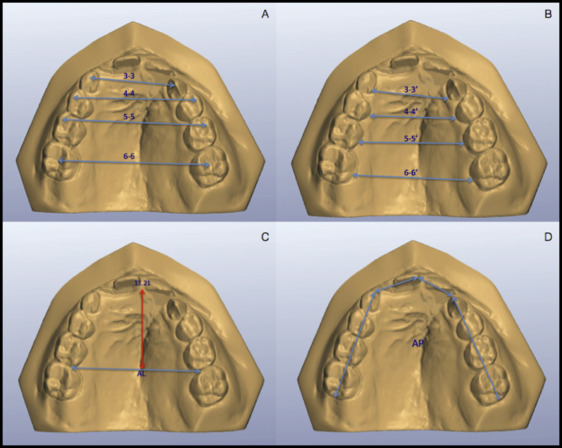
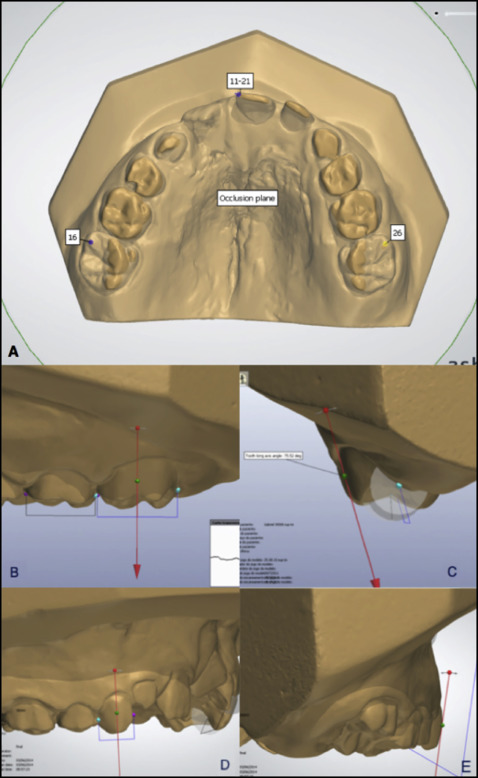
With the software OrthoAnalyzer 3D (3Shape A/S), arch widths, lengths, and perimeters were measured by 1 investigator (P.V.A.) as illustrated in Figure 2 . Palatal depth, and molar and canine inclinations were also measured using the same software ( Figs 3 , A , and 4 ). Posterior tooth inclination was measured using as the reference the occlusal plane passing through the mesiobuccal cusp tips of the maxillary first molars, bilaterally, and through a mesioincisal point on the left central incisor ( Fig 4 , A ). The tooth long axis was represented as an arrow in the virtual setup of the OrthoAnalyzer software ( Fig 4 , B and D ). On the buccal view of each posterior tooth, this arrow was mesiodistally manipulated to represent tooth angulation according to Andrews’ FA point (the most prominent part of the central lobe on each crown’s facial surface). On the distal view of each tooth, the arrow was buccolingually manipulated to represent crown torque ( Fig 4 , C and E ), according to Andrews. The angle between the arrow and the occlusal plane was automatically calculated by the software. After expansion, increasing values of the angle meant buccal inclinations of the teeth, and decreasing values meant lingual inclinations of the teeth.
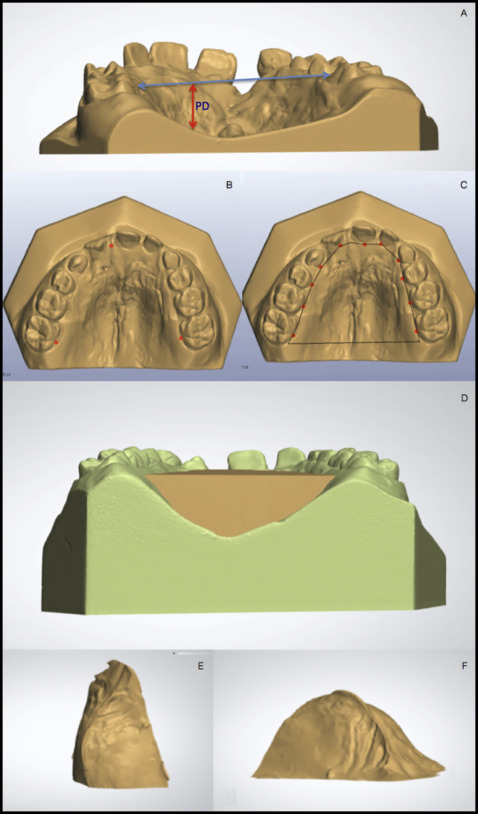
The palatal volume was measured before and after maxillary expansion using the Appliance Designer software (3Shape A/S) and the VistaDent 3D software (Materialise, Leuven, Belgium). In the Appliance Designer, a plane representing the upper limit of the palate was created passing through the lower limit of the incisal papilla and through the midpoint of the lingual gingival margin of the maxillary permanent first molars ( Fig 3 , B ). The posterior limit for the volume measurement was a plane tangent to the distal aspect of the maxillary first molars ( Fig 3 , C ). The midpoint of the lingual aspect of each maxillary tooth at the level of the gingival margin represented the lateral border for volume measurement ( Fig 3 , C ). When a tooth was totally out of the dental arch, buccally or lingually, it was not considered for the lateral demarcation of volume. A volumetric image of the palate observing the standardized borders was than created ( Fig 3 , D – F ). Volumes were calculed in cubic millimeters with the VistaDent 3D software.
Fifty percent of each group was measured twice for error analysis after a 30-day interval by the same examiner (P.V.A.). There were no discrepancies between the control and experimental group measurements. The random errors were calculated according to Dahlberg’s formula ( Se 2 = Σ d 2 /2n), where Se 2 is the error variance and d is the difference between 2 determinations of the same variable, and the systematic errors were evaluated with dependent t tests, at P <0.05.
Statistical analysis
To evaluate the comparability of the groups at the initial stage, the width measurements, arch lengths and perimeters, palatal depths and volumes, and canine, second premolar, and first molar inclinations of the groups were compared with t tests.
Intragroup treatment changes were evaluated with paired t tests. Intergroup treatment changes were compared with t tests. The statistical analyses were performed with statistical software (version 20.0; IBM, Armonk, NY). The results were considered significant at P <0.05.
Results
The random errors varied from 0.17 to 0.98 mm for the linear measurements. For the angular variables, the maximum random error was 1.05°. The random error for palatal volume corresponded to approximately 4% of the first measurements ( Table I ). Mean differences between the linear and angular measurements were smaller than 0.5 mm and 1°, respectively. No significant systematic error was found ( Table I ).
| Variable | Measurement 1 | Measurement 2 | Difference | Random errors (Dahlberg ) | Systematic errors ( P ) |
|---|---|---|---|---|---|
| Linear measurements (mm) | |||||
| 3-3′ | 27.08 | 27.22 | 0.14 | 0.89 | 0.16 |
| 3-3 | 31.4 | 31.03 | −0.37 | 0.98 | 0.27 |
| 4-4′ | 27.52 | 27.6 | 0.08 | 0.19 | 0.14 |
| 4-4 | 38.92 | 38.56 | −0.36 | 0.17 | 0.58 |
| 5-5′ | 31.11 | 31.23 | 0.12 | 0.19 | 0.77 |
| 5-5 | 43.99 | 43.61 | −0.38 | 0.34 | 0.06 |
| 6-6′ | 36.06 | 36.3 | 0.24 | 1.41 | 0.37 |
| 6-6 | 46.85 | 46.71 | −0.14 | 0.55 | 0.36 |
| Arch length | 25.58 | 24.98 | −0.6 | 0.21 | 0.12 |
| Arch perimeter | 94.95 | 95.04 | 0.09 | 0.34 | 0.35 |
| Palatal measurements (mm/mm 3 ) | |||||
| Palatal depth | 14.53 | 14.55 | 0.02 | 0.30 | 0.34 |
| Palatal volume | 2170.59 | 2218.3 | 47.71 | 94.47 | 0.44 |
| Dental tipping (°) | |||||
| Canine inclination | 64.21 | 64.33 | 0.12 | 0.42 | 0.12 |
| Second premolar inclination | 62.85 | 62.31 | −0.54 | 1.05 | 0.096 |
| First molar inclination | 75.66 | 74.77 | −0.89 | 0.62 | 0.95 |
The experimental group had significantly smaller anterior arch width, arch length, arch perimeter, and palatal volume than did the control group ( Table II ).
| Variable | Experimental group | Control group | |||||
|---|---|---|---|---|---|---|---|
| Mean T1 | SD | 95% CI | Mean T1 | SD | 95% CI | P | |
| Linear measurements (mm) | |||||||
| 3-3′ | 22.03 | 3.58 | 20.26-23.81 | 25.36 | 2.68 | 24.23-26.49 | 0.001 ∗ |
| 3-3 | 27.15 | 3.50 | 25.46-28.84 | 31.44 | 2.62 | 30.33-32.54 | 0.000 ∗ |
| 4-4′ | 24.43 | 2.92 | 23.10-25.76 | 26.75 | 1.97 | 25.90-27.55 | 0.003 ∗ |
| 4-4 | 35.64 | 3.41 | 34.09-37.20 | 37.69 | 2.77 | 36.48-38.80 | 0.030 ∗ |
| 5-5′ | 30.21 | 2.67 | 29.08-31.33 | 30.58 | 1.97 | 29.79-31.38 | 0.571 |
| 5-5 | 42.45 | 2.94 | 41.21-43.70 | 42.97 | 2.56 | 41.94-44.01 | 0.509 |
| 6-6′ | 36.09 | 3.25 | 34.75-37.43 | 35.28 | 1.92 | 34.46-36.09 | 0.289 |
| 6-6 | 45.63 | 2.70 | 44.51-46.74 | 45.37 | 2.40 | 44.36-46.39 | 0.732 |
| Arch length | 23.73 | 2.81 | 22.57-24.89 | 26.42 | 1.85 | 25.68-27.17 | 0.000 ∗ |
| Arch perimeter | 91.59 | 5.79 | 89.20-93.98 | 95.98 | 6.75 | 93.25-98.71 | 0.016 ∗ |
| Palatal measurements (mm/mm 3 ) | |||||||
| Palatal depth | 12.81 | 2.68 | 11.71-1392 | 13.49 | 1.77 | 12.78-14.20 | 0.296 |
| Palatal volume | 4796.75 | 1436.44 | 4142.89-5450.61 | 5918.20 | 1596.81 | 5286.53-6549.88 | 0.017 ∗ |
| Dental tipping (°) | |||||||
| Canine inclination | 70.42 | 9.89 | 66.15-74.70 | 73.61 | 4.55 | 72.27-74.97 | 0.186 |
| Second premolar inclination | 68.60 | 5.93 | 65.82-71.37 | 66.88 | 5.35 | 65.25-68.51 | 0.256 |
| First molar inclination | 71.18 | 6.38 | 69.30-73.05 | 70.20 | 3.74 | 67.08-73.34 | 0.557 |
In the experimental group, the expansion produced significant increases of all maxillary transverse measurements, arch perimeters, palatal volumes, and dental inclinations ( Table III ). However, there was a significant decrease of arch length.
| Variable | Preexpansion | Postexpansion | Change | P | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | Mean | SD | 95% CI | ||
| Linear measurements (mm) | ||||||||||
| 3-3′ | 22.03 | 3.58 | 20.26-23.81 | 25.96 | 3.30 | 24.32-27.60 | 3.93 | 3.00 | 2.44-5.42 | 0.000 ∗ |
| 3-3 | 27.15 | 3.50 | 25.46-28.84 | 31.07 | 3.67 | 29.30-32.84 | 3.92 | 3.07 | 2.44-5.40 | 0.000 ∗ |
| 4-4′ | 24.43 | 2.92 | 23.10-25.76 | 29.65 | 2.95 | 28.31-30.99 | 5.22 | 1.44 | 4.56-5.87 | 0.000 ∗ |
| 4-4 | 35.64 | 3.41 | 34.09-37.20 | 41.59 | 3.39 | 40.05-43.14 | 5.95 | 1.88 | 5.09-6.81 | 0.000 ∗ |
| 5-5′ | 30.21 | 2.67 | 29.08-31.33 | 35.46 | 2.47 | 34.41-36.50 | 5.25 | 1.73 | 4.52-5.98 | 0.000 ∗ |
| 5-5 | 42.45 | 2.94 | 41.21-43.70 | 48.42 | 2.71 | 47.27-49.56 | 5.97 | 1.99 | 5.12-6.80 | 0.000 ∗ |
| 6-6′ | 36.09 | 3.25 | 34.75-37.43 | 41.21 | 2.96 | 39.99-42.43 | 5.12 | 2.05 | 4.27-5.97 | 0.000 ∗ |
| 6-6 | 45.63 | 2.70 | 44.51-46.74 | 51.13 | 2.76 | 49.99-52.26 | 5.50 | 1.66 | 4.81-6.19 | 0.000 ∗ |
| Arch length | 23.73 | 2.81 | 22.57-24.89 | 22.67 | 3.09 | 21.39-23.94 | –1.06 | 1.96 | −1.87-0.25 | 0.012 ∗ |
| Arch perimeter | 91.59 | 5.79 | 89.20-93.98 | 95.24 | 5.04 | 93.16-97.32 | 3.65 | 3.99 | 2.00-5.29 | 0.000 ∗ |
| Palatal measurements (mm/mm 3 ) | ||||||||||
| Palatal depth | 12.81 | 2.68 | 11.71-1392 | 13.27 | 2.65 | 12.17-14.36 | 0.46 | 1.63 | −0.22-1.13 | 0.175 |
| Palatal volume | 4796.75 | 1436.44 | 4142.89-5450.61 | 5643.98 | 1633.16 | 4900.58-6387.38 | 847.23 | 637.93 | 556.84-1137.61 | 0.000 ∗ |
| Dental tipping (°) | ||||||||||
| Canine inclination | 70.42 | 9.89 | 66.15-74.70 | 74.00 | 7.88 | 70.60-77.41 | 3.58 | 7.30 | 0.43-6.74 | 0.028 ∗ |
| Second premolar inclination | 68.60 | 5.93 | 65.82-71.37 | 71.26 | 4.93 | 68.95-73.56 | 2.66 | 5.15 | 0.25-5.07 | 0.032 ∗ |
| First molar inclination | 71.18 | 6.38 | 69.30-73.05 | 73.35 | 7.24 | 71.23-75.48 | 2.17 | 5.27 | 0.63-3.72 | 0.007 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


