Key points
- •
The upper facial region frames the eyes and thus has been one of major hallmarks of beauty for millennia.
- •
Cosmetic surgery in the region is one of most rewarding and sought after surgeries in the discipline.
- •
Evaluation, analysis, and diagnosis is of utmost importance in achieving optimal results; however, there is constant debate over the ideal method of analysis.
- •
The surgical management of this region is continually evolving in hopes of achieving the ideal result and ultimate patient and surgeon satisfaction.
- •
Preoperative planning is of utmost importance in minimizing postoperative complications.
Introduction
Facial esthetic analysis has a long and fundamental history in cosmetic surgery. There is continual debate on what is deemed to be esthetic and it continues to evolve. In addition, the views on facial esthetics can vary between ethnicities, cultures, geographies, and fashion trends. However, there are many key concepts that have not changed in centuries. Furthermore, the surgical intervention used to restore and improve facial esthetics is constantly evolving. The ideal assessment of beauty is a balance between the desires and wishes of a patient and his or her surgeon. The ultimate success is measured by a patient’s satisfaction.
Introduction
Facial esthetic analysis has a long and fundamental history in cosmetic surgery. There is continual debate on what is deemed to be esthetic and it continues to evolve. In addition, the views on facial esthetics can vary between ethnicities, cultures, geographies, and fashion trends. However, there are many key concepts that have not changed in centuries. Furthermore, the surgical intervention used to restore and improve facial esthetics is constantly evolving. The ideal assessment of beauty is a balance between the desires and wishes of a patient and his or her surgeon. The ultimate success is measured by a patient’s satisfaction.
Patient evaluation
Patient evaluation is a very important aspect of the analysis of a potential cosmetic surgery patient. A thorough history and physical should be performed on all preoperative patients. In addition to the standard history and physical examination, a focused review of systems should be performed with focus of facials issues like vision changes, dry eyes, and so on. In addition, particular attention should be addressed to the use of over-the-counter supplements because they can alter healing and coagulation and thus have impact on surgical outcomes and incidence of complications.
The most critical aspect of the patient evaluation in the cosmetic surgery patient is obtaining a detailed chief complaint. Even if the surgical outcome of cosmetic surgery is outstanding, if it does not address the chief complaint, the final outcome is a failure. In some cases, the chief complaint may need to be modified by the patient, once the patient is counseled on the areas of interest. In addition, the patient’s motivation for undergoing surgery is of critical significance; internal patient motivation will typically lead to highest rate of success. In cases where patient motivations are questionable or their expectations are not realistic, the ideal success may be referral of the patient to a different provider!
Photo documentation
Photo documentation is of critical importance in cosmetic surgery. It aids not only in the analysis and diagnosis of patients, but also serves to educate patients on the findings. Furthermore, not only can these photos help to educate the patient preoperatively, they can help to educate and inform patient postoperatively, particularly when patients are dissatisfied with their results. It is beyond the scope of this paper to discuss photo documentation in detail. The keys for successful photo documentation are taking all photos for all patients in the same fashion and same angle. For the face, it is particularly important to take photos with and without a flash to help accentuate shadows and contour deformities that one wishes to improve or correct surgically. If preoperative and postoperative photos are taken with a flash only, the before and after photos will not do justice to the true result achieved. This may become less of an issue as 3-dimensional photography becomes more common.
Anatomic analysis
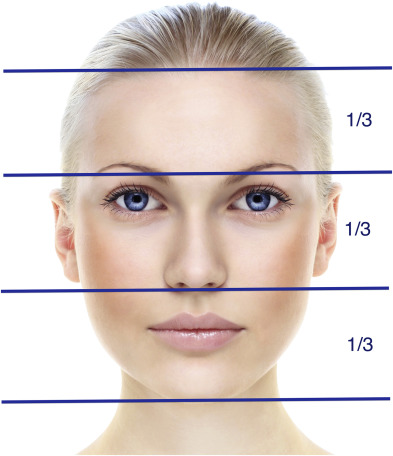
Traditionally, when analyzing the face in the vertical dimension, it is divided equally into thirds ( Fig. 1 ). When dividing the facial height into thirds vertically, the top third extends form the hairline to glabella, the middle third extends from the glabella to the subnasale, and the lower third extends from the subnasale to menton.
When analyzing the face in the horizontal dimension, it is divided equally in fifths ( Fig. 2 ). The facial width is divided in fifths horizontally, the most lateral fifth extends from the pinna to the lateral canthus, the central fifth extends from medial canthus to medial, and the other fifth is the palpebral third, which extends form lateral canthus to the medial canthus. In addition, with analyzing the horizontal dimensions, it is considered balanced when the intercanthal distance is coincident with the alar bases.
It is considered esthetic when there is quantitative equality between these vertical thirds and horizontal fifths. Facial shapes arise from the interplay between the ratio of the facial thirds and fifths to each other. For example, longer faces will have longer facial thirds in comparison with the facial fifths.
In general, the face should have smooth flowing contours and these should be smooth and contiguous or complementary with adjacent facial areas. For example, the orbital rim continues a smooth flowing contour to the lateral aspect of the nose and the lower eyelid blends gently into the midface on a profile view.
Esthetic analysis by region
Forehead
The hairline can change overtime and thus its esthetic position does not always follow the “rule of thirds” for the face. The other method used is the “curve of the head rule” and using the line drawn between the intersection of the horizontal line of the scalp with vertical line of the face. Thus, the hairline rests somewhere on the curve joining these 2 planes. In general, the hairline should be located 5 to 6 cm (5 cm in females and 6 cm in males) from the brow, in a patient with a nonreceded hairline.
Forehead convexity and inclination can play a significant role in the perceived forehead height. A patient with a flat or protruding forehead will have an apparent shorter forehead compared with that of patient with a posteriorly sloping forehead. In addition, recognizing the inclination of the forehead, its length, and the position of the hairline are important in preoperative planning of endoscopic procedures in the area. In general, ideal esthetics are seen with a forehead having a gently convex surface extending from the top of head to the brow (on a profile view). The most anterior aspect of the forehead should be at the glabella just above the nasion. The nasofrontal angle should be 115° to 135°.
The prominence of the glabella and overlying soft tissues is quite important to forehead esthetics as well. The prominence is typically more profound in the male patient. Thus, many females with prominence in the area request the prominence to be addressed surgically. A lateral cephalometric radiograph can be useful in assessing bony contours in the area and for surgical planning should glabellar reduction be performed. Modification of the glabella and supraorbital ridge can play a very important role in the cosmetic surgery patient, particularly in facial feminization procedures. If glabellar prominence is seen in combination with deep static glabeller rhytids and accentuated volume on dynamic contraction, the excess volume is likely from muscular hypertrophy. This muscular hypertrophy can be address through surgical excision or the use of neuromodulators.
Analysis of forehead static and dynamic rhytids are an important part of the facial analysis as well. Static rhytids develop over time in the forehead from contraction of the frontalis muscle from raising the brow. Rhytids over the glabella and nasal dorsum are from contraction of the corrugator supercilli muscle and procerus muscle. Dynamic rhytids can typically be addressed with neuromodulators or surgery; however, deeper static rhytids typically require operative intervention and skin resurfacing and possible volume augmentation.
Eyebrow
The eyebrows are defined by the hair growth in the area. In general, in the esthetic brow, the brow hairs have a general angle of orientation at the different aspects of the brow, at its most medial aspect the hair is oriented in superior direction and are then directed more laterally in the central brow and then continue to follow in parallel with the course of the brow. With the degree of grooming that occurs in the area, the amount of hair remaining in the area is sometimes negligible, hence the increased amount of eyebrow tattooing seen in current times. These patients can sometimes be challenging to treat, particularly if the tattooing is placed at a higher level than where the native brow used to be.
The ideal brow architecture and position has been described by Westmore. He described the brow ( Fig. 3 ) as beginning medially along a vertical line running from nasal ala and medial canthus. The brown terminates laterally on the line running from the nasal ala to the lateral canthus. The peak of the arch of brow was described as being centered over a vertical line drawn from the lateral corneal limbus. This has been modified by many and there are number of other descriptions with slight variation, most notable being the peak of the arch being centered anywhere from the lateral limbis to the lateral canthus. Some studies have shown there to be no superior esthetic brow architecture. However, other studies have shown some brow architectures to be more esthetically pleasing, particularly when comparing different facial shapes.
The ideal esthetic brow definition changes with age, sex and ethnicity. The ideal brow height also differs at different aspects of the brow. Further complicating the matter are culture and current fashion trends, and the resulting grooming of the eyebrow can alter the natural brow position significantly. Classically, the medial brow starts at or above the orbital rim and then arches superiorly moving laterally. The height of the arch is typically anywhere from the lateral corneal limbus to lateral canthus. However, in the male brow, there is typically less or an arch and it is positioned mostly over the orbital rim ( Fig. 4 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


