Introduction
This was a cross-sectional study to investigate the agreement between assessments of orthodontic treatment need of the index of complexity, outcome, and need (ICON) and the index of orthodontic treatment need (IOTN).
Methods
Five hundred two subjects (253 girls, 249 boys; ages, 11–14 years) participated in this study, including a few who were wearing an orthodontic appliance (1 girl, 5 boys). ICON scores and the aesthetic (AC) and dental health components (DHC) of the IOTN were recorded in those not undergoing treatment. The percentages of subjects needing treatment (ICON score >43) and the different complexity components of ICON were compared between the sexes. Observed percentages of agreement and kappa statistics were used to analyze the agreement between the AC and DHC of the IOTN and also the ICON, and the DHC and AC of the IOTN dichotomized into a yes or no categories of orthodontic treatment need.
Results
No sex differences were found between male and female subjects for treatment need (ICON score >43; P >0.05) and treatment complexity ( P >0.05). The kappa statistic for diagnostic agreement between the DHC and AC of the IOTN was 0.55 (95% CI, 0.48–0.63). The kappa statistics for diagnostic agreement between the ICON and the AC and the DHC of the IOTN were 0.40 (95% CI, 0.33–0.46) and 0.78 (95% CI, 0.73–0.83), respectively. The observed agreement between the DHC and the AC of the IOTN was 81.8%. The observed agreement between the ICON and AC and DHC of the IOTN were 71.3% and 89.5%, respectively.
Conclusions
In terms of orthodontic treatment need, there was moderate agreement between the ICON and the AC (IOTN), and between the DHC and the AC. There was good agreement between the ICON and the DHC of the IOTN. The ICON is a good substitute for the DHC of the IOTN.
Orthodontic indexes were developed to standardize the assessment of orthodontic care. This in theory helps the specialty to allocate limited resources, identify the most effective appliances, and increase the professional esteem among involved clinicians. The oral health benefits of orthodontic intervention are quite limited, and previous studies have stated that the main ill effect of malocclusion is psychosocial and related to esthetic impairment, rather than any functional disadvantages. In this context, any index should theoretically have an assessment of esthetics integrated into it, even though the psychological health gain from orthodontic treatment has been disputed recently.
Several orthodontic indexes have been proposed to provide information on the prevalence of malocclusions and objectively quantify the severity of the various features of malocclusion. The index of orthodontic treatment need (IOTN), and the index of complexity, outcome, and need (ICON) are perhaps the most commonly used orthodontic indexes. These indexes both have esthetic components and intend to measure the severity of the malocclusion objectively, either as a deviation from normal occlusion or in terms of perceived treatment need. Usually for these indexes of treatment need, there is a system of protocols to summarize the data about the malocclusion and return a numeric value. In identifying those needing and not needing orthodontic treatment, there are cutoff points. In each index, there is a numeric value below which the severity of a malocclusion is considered so minor that treatment is not needed. All numeric values above that point indicate malocclusions for which treatment is indicated. Cutoff points for eligibility to receive treatment in publicly funded programs can be modified to meet the available resources, and different cutoff points will identify different proportions of the population requiring orthodontic treatment.
Orthodontic indexes have enabled us to quantify the need for treatment; however, they are not always comparable. This is particularly important when comparing the previous epidemiologic studies with different orthodontic indexes. The aim of this cross-sectional study was to investigate the diagnostic agreement between assessments of orthodontic treatment need of an 11- to 14-year-old population by using the ICON and the Dental Health (DHC) and Aesthetic (AC) components of the IOTN.
Material and methods
This research was approved by the Research Ethics Committee and the Faculty of Community Dentistry, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran.
This cross-sectional study was originally carried out to provide preliminary information on the prevalence of malocclusions and occlusal traits in Iranian school children. The target population consisted of urban schoolchildren aged 11 to 14 years in Isfahan, Iran. This age group represents the period of eruption of the permanent canines and premolars when most potential orthodontic problems become evident. Isfahan is the capital city of Isfahan Province and Iran’s third largest city. It is located in the central part of Iran with 3% of the whole population. The city had a population of 1,986,542, and the Isfahan metropolitan area had a population of 3,430,353 in the 2006 census, the second most populous metropolitan area in Iran after the capital.
The exclusion criteria for this study were subjects with craniofacial anomalies (clefts and syndromes) and non-Iranian nationals. To ensure a random selection from the schools, 6 public schools were randomly selected from different geographic locations in Isfahan. A total of 502 subjects participated in this study; however, 6 subjects (1 girl, 5 boys) had previous orthodontic treatment and were excluded. Consequently, 496 subjects were included in the study (244 boys, 252 girls).
The IOTN categorizes malocclusion in terms of the significance of various occlusal traits for a person’s dental health and perceived esthetic impairment, with the intention of identifying those who would most likely benefit from orthodontic treatment. The index has 2 components: the AC and the DHC. The AC consists of 10 color photographs showing different levels of dental attractiveness, with grade 1 representing the most attractive and grade 10 the least attractive dentitions. The DHC incorporates the various occlusal traits considered to increase the morbidity of the dentition. There are 5 grades in the DHC that have been grouped after validation into grades 1 and 2 representing no need for treatment, grade 3 representing borderline cases, and grades 4 and 5 representing those who need orthodontic treatment.
The ICON was developed based on the average opinions of 97 practicing specialist orthodontists from 9 countries. It is a single assessment method to quantify orthodontic treatment complexity, outcome, and need. The ICON is unique in incorporating an esthetic score (similar to the AC of the IOTN) as an integral part of the evaluation of treatment need. Because it is both an index of treatment need and an occlusal index of malocclusion severity, the ICON offers significant advantages over other indexes of treatment need. The ICON consists of 5 components: the esthetic component, maxillary and mandibular crowding or spacing assessment, presence of a crossbite, degree of incisor open bite or overbite, and fit of the teeth in the buccal segment in terms of the anteroposterior relationship. Each component can be measured on study casts and on patients. The practical application of the index is simple and takes approximately 1 minute for each patient.
An orthodontist (first author, A.B.F.), who had been formally trained and calibrated in the use of the IOTN and the ICON, visited the schools and conducted the clinical examinations. A mouth mirror, a ruler, and a digital sliding calipers were used.
Statistical analysis
All the data were collected and entered into the Statistical Package for Social Sciences program for statistical analysis (version 17, SPSS, Chicago, Ill). Descriptive statistics such as means and standard derivations were calculated in the data analysis. Confidence intervals were calculated for average ICON scores in both sexes. The proportions of subjects of each sex needing treatment, as defined by having an ICON score of at least 44, were compared by using the chi-square test. The numbers of subjects in each ICON component (easy, mild, moderate, difficult, and very difficult) were compared according to sex with the chi-square test.
Observed percentage agreement and kappa statistics were used to analyze the agreement between the DHC and the AC of the IOTN dichotomized into a yes or no category of orthodontic treatment need. Observed percentage agreement and kappa statistics were also used to analyze the agreement between the ICON and the DHC and the AC of the IOTN dichotomized into a yes or no category of orthodontic treatment need. The level of agreement was defined by using the following scale (Altman ): poor agreement, less than 0.20; fair agreement, 0.20 to 0.40; moderate agreement, 0.40 to 0.60; good agreement, 0.60 to 0.80; and very good agreement, 0.80 to 1.00. Any P values less than 0.05 were interpreted as statistically significant.
Results
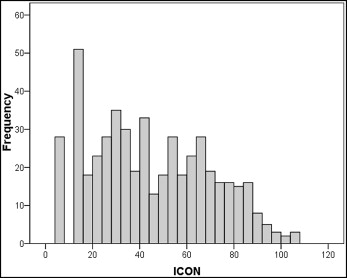
The mean ICON score was 44.6 points (95% CI, 42.41–46.79). The mean ICON scores for male and female subjects were 46.81 ± 24.75 (SD) and 42.46 ± 24.78 (SD), respectively, as shown in Table I . Figure 1 shows the histogram of ICON scores.
| ICON scores | Mean | SD | 95% CI |
|---|---|---|---|
| Boys (n = 244) | 46.81 | 24.75 | 43.69–49.93 |
| Girls (n = 252) | 42.46 | 24.78 | 39.39–45.54 |
| Total | 44.60 | 24.83 | 42.41–46.79 |
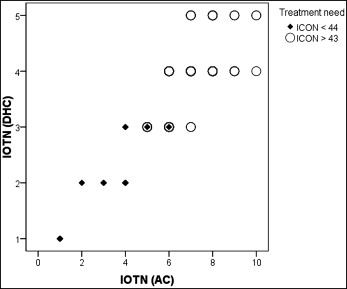
The need for orthodontic treatment, according to an ICON score of at least 44, was 46.6%. In terms of orthodontic treatment need, 46.7% of the boys needed treatment, compared with 46.4% of the girls; the difference was not significant ( Table II ). Table III summarizes the distribution of subjects in the treatment complexity compartments. In terms of complexity, a higher proportion of boys was in the very difficult compartment (14.8%) compared with the girls (9.1%). Overall, the degree of complexity did not vary significantly between the sexes ( P >0.05). In assessing treatment complexity, only 26.4% of the subjects were considered difficult or very difficult. According to the AC and the DHC of the IOTN, 17.9% and 36.1% of the subjects showed a definite need for orthodontic treatment, respectively ( Table IV ). Figure 2 shows the relationship between the DHC and the AC of the IOTN according to ICON scores of at least 44.
| Treatment need ∗ | Male | Female | Total |
|---|---|---|---|
| No need for treatment | |||
| ICON <44 | 130 (53.3%) | 135 (53.6%) | 265 (53.4%) |
| Treatment needed | |||
| ICON ≥44 | 114 (46.7%^) | 117 (46.4%) | 231 (46.6%) |
| Total | 244 | 252 | 496 |
| ICON complexity grade ∗ | Male | Female | Total |
|---|---|---|---|
| Easy | |||
| <29 | 73 (29.9%) | 94 (37.3%) | 167 (33.7%) |
| Mild | |||
| 29–50 | 67 (27.5%) | 56 (22.2%) | 123 (24.8%) |
| Moderate | |||
| 51–63 | 32 (13.1%) | 43 (17.1%) | 75 (15.1%) |
| Difficult | |||
| 64–77 | 36 (14.8%) | 36 (14.3%) | 72 (14.5%) |
| Very difficult | |||
| >77 | 36 (14.8%) | 23 (9.1%) | 59 (11.9%) |
| Total | 244 | 252 | 496 |
| IOTN | Male | Female | Total |
|---|---|---|---|
| AC | |||
| 1–4 | |||
| No or little need | 111 (45.5%) | 117 (46.4%) | 228 (46%) |
| 5–7 | |||
| Borderline need | 89 (36.5%) | 90 (35.7%) | 179 (36.1%) |
| 8–10 | |||
| Definite need | 44 (18%) | 45 (17.9%) | 89 (17.9%) |
| DHC | |||
| 1 & 2 | |||
| No or little need | 106 (43.4%) | 111 (44%) | 217 (43.8%) |
| 3 | |||
| Borderline need | 47 (19.3%) | 53 (21%) | 100 (20.2%) |
| 4 & 5 | |||
| Definite need | 91 (37.3%) | 88 (34.9%) | 179 (36.1%) |
| Total | 244 | 252 | 496 |
When we assessed agreement between the DHC and the AC of the IOTN, the kappa statistic for the diagnostic agreement was 0.55 (95% CI, 0.48–0.63), indicating moderate agreement. When we assessed agreement between the ICON and AC and DHC of the IOTN, the kappa statistics for the diagnostic agreement were 0.401 (95% CI, 0.33–0.46) and 0.786 (95% CI, 0.73–0.83), respectively. These values indicate moderate and good levels of agreement, respectively ( Table V ). The observed percentage of agreement between the DHC and the AC of the IOTN was 81.8%. The observed percentages of agreement between the ICON and the AC and the DHC of the IOTN were 71.3% and 89.5%, respectively.


