Introduction
Our aims were to analyze adhesion of periodontopathogens to self-ligating brackets (Clarity-SL [CSL], Clippy-C [CC] and Damon Q [DQ]) and to identify the relationships between bacterial adhesion and oral hygiene indexes.
Methods
Central incisor brackets from the maxilla and mandible were collected from 60 patients at debonding after the plaque and gingival indexes were measured. Adhesions of Aggregatibacter actinomycetemcomitans (Aa), Porphyromonas gingivalis (Pg), Prevotella intermedia (Pi), Fusobacterium nucleatum (Fn), and Tannerella forsythia (Tf) were quantitatively determined using real-time polymerase chain reactions. Factorial analysis of variance was used to analyze bacterial adhesion in relation to bracket type and jaw position. Correlation coefficients were calculated to determine the relationships between bacterial adhesion and the oral hygiene indexes.
Results
Total bacteria showed greater adhesion to CSL than to DQ brackets, whereas Aa, Pg, and Pi adhered more to DQ than to CSL brackets. CC brackets showed an intermediate adhesion pattern between CSL and DQ brackets, but it did not differ significantly from either bracket type. Adhesion of Fn and Tf did not differ significantly among the 3 brackets. Most bacteria were detected in greater quantities in the mandibular than in the maxillary brackets. The plaque and gingival indexes were not strongly correlated with bacterial adhesion to the brackets.
Conclusions
Because Aa, Pg, and Pi adhered more to the DQ brackets in the mandibular area, orthodontic patients with periodontal problems should be carefully monitored in the mandibular incisors where the distance between the bracket and the gingiva is small, especially when DQ brackets are used.
Highlights
- •
We compared periodontal pathogens on various anterior self-ligating brackets.
- •
Mandibular brackets held more periodontal pathogens than maxillary brackets.
- •
More pathogens adhered to Damon Q than to Clarity-SL.
- •
Clippy-C showed an intermediate adhesion pattern.
- •
Oral hygiene indexes were not strongly associated with bacterial adhesion to brackets.
Bacterial compositions around orthodontic appliances change dynamically during orthodontic treatment with fixed appliances. One change is excessive growth of putative periodontal pathogens around orthodontic appliances. Increased composition of periodontal pathogens induces gingival inflammation by the interactions between the pathogens and host tissues. Although gingival inflammation decreases after removing the fixed appliances, the relationships between fixed orthodontic appliances and periodontal problems require further study.
Gram-negative anaerobes, such as Aggregatibacter actinomycetemcomitans (Aa), Fusobacterium nucleatum (Fn), Porphyromonas gingivalis (Pg), Prevotella intermedia (Pi), and Tannerella forsythia (Tf), are well known as putative periodontal pathogens. In particular, the presence of red complex species—Pg and Tf—in biofilms is strongly associated with gingival health, and orange complex species—Pi and Fn—are considered to be bridge bacteria between early colonizers and the red complex species.
Among various orthodontic appliances, brackets may play a significant role in gingival inflammation because they attach to the dentition close to the gingival tissues, and their complex designs can interfere with proper access to the tooth surfaces for cleaning. As a result, brackets may promote plaque accumulation, adhesion of periodontal pathogens, and pathologic changes such as gingivitis, gingival bleeding, and gingival enlargement around them.
Recently, self-ligating brackets have been introduced in clinical orthodontics. Self-ligating brackets have many advantages, such as elimination of the elastomeric or stainless steel ligature, reduced complexity, and fewer retentive sites for bacterial adhesion, which may facilitate better oral hygiene. Since in-vitro and in-vivo studies have shown differences in bacterial adhesion among various brackets, especially for cariogenic streptococci, bracket types may have different effects on the adhesion of periodontal pathogens.
The latest molecular approaches have increased the detection of periodontal pathogens that adhere to dental materials. Real-time polymerase chain reaction (PCR) is particularly suited for identifying periodontal pathogens because this rapid procedure has higher sensitivity and fewer risks of contamination compared with conventional culture procedures. The aim of this in-vivo prospective study was to quantitatively analyze adhesion of periodontal pathogens to different self-ligating brackets using real-time PCR. A secondary aim was to identify relationships between adhesion of periodontal pathogens and oral hygiene indexes. The null hypotheses of this study were that there would be no significant difference in adhesion of periodontal pathogens among different self-ligating brackets, and no significant relationships would be found between adhesion of periodontal pathogens and oral hygiene indexes. To our knowledge, this is the first in-vivo study to investigate the adhesion of various periodontal pathogens to self-ligating brackets with real-time PCR.
Material and methods
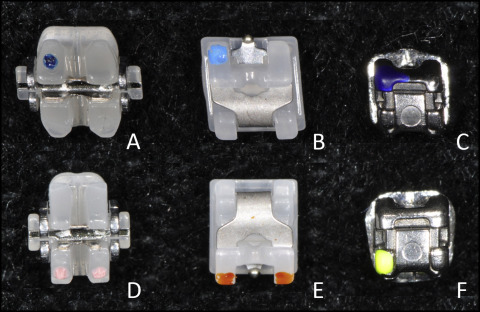
The study population consisted of adult patients who were planning to finish orthodontic treatment with fixed appliances. Inclusion criteria at the start of this experiment were (1) ages greater than 19 years for the male patients and 17 years for the female patients, (2) a treatment period longer than 12 months (mean, 20.1 months), and (3) use of one of three bracket types with a 0.022-in slot: Clippy-C (CC; Tomy, Tokyo, Japan), Clarity SL (CSL; 3M Unitek, Monrovia, Calif), and Damon Q (DQ; Ormco, Orange, Calif) ( Fig 1 ). Exclusion criteria were (1) any systematic disease, (2) any active carious lesions, (3) topical fluoride application (except for a fluoridated dentifrice) or antibacterial therapy within 6 months, and (4) use of elastomeric chains or stainless steel ligatures before sample collection. All subjects signed informed consent forms, and the institutional review board of Seoul National University Dental Hospital, Seoul, Korea, approved the study protocol.
Power analysis was performed for the estimation of effect size using information from previous studies. The analysis indicated that at least 34 brackets per group were needed for statistical power close to 0.8 at α = 0.05. We collected 244 brackets (CC brackets, 84; CSL brackets, 88; DQ brackets, 68) from 60 subjects (CC, 21 subjects; CSL, 22 subjects; and DQ, 17 subjects), including 21 men and 39 women with a mean age of 23.5 years.
All subjects were asked to refrain from eating, brushing their teeth, and rinsing their mouth for at least 2 hours before debonding. At debonding, the maxillary and mandibular left and right central incisor brackets (4 brackets per patient) were collected immediately after 1 investigator (W-S.J.) determined the plaque index and the gingival index for the same teeth, and the simplified oral hygiene index. The simplified oral hygiene index assesses oral hygiene status by measuring debris and calculus deposition from 2 anterior and 4 posterior teeth. The plaque index is a categorical scale in which 0 indicates no plaque accumulation; 1 indicates invisible plaque adhering to the tooth that can be scraped with only a probe; 2 indicates moderate accumulation that can be seen with the naked eye; and 3 indicates abundant accumulation. The gingival index is a categorical scale in which 0 indicates no abnormal status of the gingiva; 1 indicates mild inflammation but no bleeding on probing; 2 indicates moderate inflammation with bleeding on probing; and 3 indicates severe inflammation with a tendency to spontaneously bleed.
All laboratory data were collected using a coding system to ensure a blind experiment. As soon as the brackets were collected, they were washed with 1.0 mL of cold phosphate-buffered saline solution (pH = 7.4) to remove unbound bacteria. Each bracket was then placed in a round tube with 2.0 mL of cold phosphate-buffered saline solution and homogenized by sonication with 3 pulses (for 30 seconds with 30-second intermittent cooling stages) in a chilled icebox. The bracket was removed from the tube, and the contents of the tube were centrifuged at 13,000 revolutions per minute for 10 minutes. The pellet was then subjected to DNA extraction.
Bacterial chromosomal DNA was extracted using a CellEase Bacteria II Genomic DNA extraction kit (Biocosm, Osaka, Japan) according to the manufacturer’s instructions. The DNA was then purified by phenol-chloroform extraction and ethanol precipitation. A NanoVue spectrophotometer (General Electric Healthcare Life Sciences, Pittsburgh, Pa) was used to assess the quality of the extracted DNA after preparation.
Known specific primers that amplify the RNA polymerase β subunits of Aa, Fn, and Tf were used. The PCR primers of Pi and Pg were designed based on the 16S rRNA gene ( Table I ). A conserved sequence in the 16S rRNA gene was selected to quantify the numbers of total bacteria. All primers were commercially synthesized (Bioneer, Seoul, Korea).
| Primer | Primer sequence (5′- to -3′) | Size of amplicon (bp) |
|---|---|---|
| Universal | F: TGGAGCATGTGGTTTAATTCGA | 160 |
| R: TGCGGGACTTAACCCAACA | ||
| Aa | F: GGCGAGCCTGTATTTGATGTGCG | 113 |
| R: GTGCCCGGTGCTGCGTCTTTG | ||
| Fn | F: ACCTAAGGGAGAAAC AGA ACC A | 171 |
| R: CCTGCCTTTAATTCATCTCCAT | ||
| Pi | F: AATACCCGATGTTGTCCACA | 337 |
| R: TTAGCCGGTCCTTATTCGAA | ||
| Pg | F: TGCAACTTGCCTTACAGAGGG | 344 |
| R: ACTCGTATCGCCCGTTATTC | ||
| Tf | F: CGGGCGTGCATCTTGTCGTCTAC | 134 |
| R: CTTAACCGGCCGCCTCTTTGAA |
Bacterial chromosomal DNA was extracted from Aa ATCC 43718, Fn ATCC 10953, Pi ATCC 25611, Pg ATCC 33277, and Tf ATCC 43037 using a G-spin Genomic DNA extraction kit (iNtRON Biotechnology, Seoul, Korea) according to the manufacturer’s instructions. The DNA standard curve consisted of known amounts of molecules of purified PCR products. The PCR products were isolated from the agarose gels using a QIAquick Gel extraction kit (Quiagen, Duesseldorf, Germany) according to the manufacturer’s instructions. DNA concentration was estimated by absorbance at 260 nm, and a series of 10-fold dilutions was prepared for standard curves as described previously. The amounts of bacterial DNA in the samples were estimated from the standard curve.
Real-time PCR was performed using the Bio-Rad iQ5 system (Bio-Rad, Hercules, Calif). The reaction mixtures contained 2 μL of purified DNA from saliva samples, 10 pM primers, and 10 μL of 2x iQ SYBR Green Supermix (Bio-Rad). Distilled water was added to obtain a final volume of 20 μL. The cycling conditions were as follows: for universal primers, initial denaturation for 30 seconds at 94°C, 40 cycles of denaturation for 20 seconds at 95°C, primer annealing for 45 seconds at 60°C, and extension for 10 seconds at 60°C; initial denaturation for 10 minutes at 95°C, 40 cycles of denaturation for 10 seconds at 95°C, primer annealing and extension for 30 seconds at 72°C for Aa 16 and Tf primers, and at 66°C for Fn primers ; for Pi and Pg primers, initial denaturation for 1 minute at 95°C, 40 cycles of denaturation for 5 seconds at 95°C, primer annealing for 15 seconds at 61°C, and extension for 33 seconds at 72°C, and final extension for 10 minutes at 72°C. All data were analyzed using the iQ5 Optical System software (Bio-Rad). The experiments to quantify the levels of bacteria were performed in triplicate and were independently repeated twice.
Statistical analysis
Differences in the amounts of bacterial adhesion in relation to bracket type and jaw position were determined using 2-way factorial analysis of variance (ANOVA) after a log transformation of the amounts of bacteria. Spearman rank correlation coefficients were used to determine the relationships between bacterial adhesion and the oral hygiene indexes on the same tooth. P values less than 0.05 were considered statistically significant.
Results
Primer specificities were tested using 18 strains of gram-positive and gram-negative species ( Table II ). During primer specificity testing, bacterial genomic DNA showed a specific DNA band around 160 base pairs (bp) with a universal primer set. For the specific primers, each periodontal pathogen produced a specific DNA fragment that was not detected in other species (data not shown).
| Gram-positive bacteria | Gram-negative bacteria |
|---|---|
| Actinomyces naeslundii KCOM 1472 | Aggregatibacter actinomycetemcomitans ATCC 33384 |
| Lactobacillus rhamnosus ATCC 7469 | Fusobacterium nucleatum ATCC 10953 |
| Streptococcus gordonii ATCC 10558 | Neisseria subflava ATCC 49275 |
| Streptococcus mutans UA159 | Porphyromonas gingivalis ATCC 33277 |
| Streptococcus oralis ATCC 9811 | Prevotella intermedia ATCC 25611 |
| Streptococcus rattus BHT | Prevotella nigrescens ATCC 33563 |
| Streptococcus salivarius CCUG 50207 | Tannerella forsythia ATCC 43037 |
| Streptococcus sanguinis CCUG 17826 | Treponema denticola ATCC 33521 |
| Streptococcus sobrinus SL1 | Veillonella dispar KCOM 1864 |
Table III and Figure 2 show the differences in adhesion of total bacteria, Aa, Fn, Pg, Pi, and Tf, in relation to bracket type and jaw position. The results of the factorial ANOVA showed that the main factors, such as bracket type and jaw position, had significant effects on bacterial adhesion without interaction effects.
| CC (n = 84) | CSL (n = 88) | DQ (n = 68) | Significance ∗ | ||||
|---|---|---|---|---|---|---|---|
| Mx (n = 42) | Mn (n = 42) | Mx (n = 44) | Mn (n = 44) | Mx (n = 34) | Mn (n = 34) | ||
| Total bacteria (log 10 /mL) | 8.67 ± 0.29 | 8.95 ± 0.55 | 8.83 ± 0.42 | 8.99 ± 0.40 | 8.59 ± 0.29 | 8.86 ± 0.24 | CSL > DQ † Mx < M n † |
| Aa (log 10 /mL) | 2.50 ± 0.75 | 2.45 ± 0.70 | 2.54 ± 0.78 | 2.56 ± 0.54 | 2.71 ± 0.75 | 2.93 ± 0.69 | CC or CSL < DQ † Mx = Mn |
| Fn (log 10 /mL) | 4.38 ± 0.90 | 4.98 ± 0.55 | 4.32 ± 0.98 | 4.82 ± 0.96 | 4.43 ± 0.76 | 4.94 ± 0.75 | CC = CSL = DQ Mx < Mn † |
| Pg (log 10 /mL) | 2.28 ± 0.87 | 2.63 ± 1.33 | 2.18 ± 0.72 | 2.39 ± 0.99 | 2.35 ± 0.79 | 3.02 ± 1.20 | CSL < DQ ‡ Mx < Mn † |
| Pi (log 10 /mL) | 2.31 ± 1.11 | 2.79 ± 1.40 | 2.17 ± 1.03 | 2.52 ± 1.12 | 2.71 ± 1.65 | 2.87 ± 1.24 | CSL < DQ § Mx < Mn ‡ |
| Tf (log 10 /mL) | 0.82 ± 0.97 | 1.31 ± 1.45 | 1.24 ± 1.26 | 1.63 ± 1.45 | 1.00 ± 1.08 | 1.27 ± 1.43 | CC = CSL = DQ Mx < Mn ‡ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


