Introduction
A digital analysis that is shown to be accurate will ease the demonstration of initial case complexity. To date, no literature exists on the accuracy of the digital American Board of Orthodontics Discrepancy Index (DI) calculations when applied to pretreatment digital models.
Methods
Plaster models were obtained from 45 previous patients with varying degrees of malocclusion. Total DI scores and the target disorders were computed manually with a periodontal probe on the original plaster casts (gold standard) and digitally using Ortho Insight 3D (Motion View Software, Hixson, Tenn) and OrthoCAD (Cadent, Carlstadt, NJ). Intrarater and interrater reliabilities were assessed for 15 subjects using the Spearman rho correlation test. Accuracies of the DI scores and target disorders were assessed for all 45 subjects using Wilcoxon signed ranks tests.
Results
Intrarater and interrater reliabilities were high for total DI scores and most target disorders ( r > 0.8). No significant difference was found between total DI score when measured with OrthoCAD compared with manual calculations. The total DI scores calculated by Ortho Insight 3D were found to be significantly greater than those by manual calculation by 2.71 points.
Conclusions
The findings indicate that a DI calculated by Ortho Insight 3D may lead the clinician to overestimate case complexity. OrthoCAD’s DI module was demonstrated to be a clinically acceptable alternative to manual calculation of the total scores.
Highlights
- •
We measured ABO discrepancy index (DI) digitally and on plaster casts.
- •
Total DI scores with OrthoCAD and plaster measurements were similar.
- •
Total DI score with Ortho Insight 3D was significantly larger than plaster casts.
- •
With OrthoCAD, only the overjet measurement differed from the plaster casts.
- •
With Ortho Insight 3D, multiple measurements differed.
Digital technology has become an integral component in orthodontic offices. Its use meets the demands of multiple-doctor practices, multiple practice locations, and increases in the patient base and allows efficient and convenient storage, retrieval, and sharing of information. For dental model analysis, plaster models have been the gold standard, but they are subject to loss, fracture, and degradation; are difficult to retrieve and share; and require physical storage space. To overcome these problems, 3-dimensional (3D) study models have increased in popularity. In addition to being an essential component of initial diagnosis and treatment planning, objective model analysis is necessary for demonstrating case complexity for those pursuing certification by the American Board of Orthodontics (ABO). The ABO devised the Discrepancy Index (DI) to provide an objective method to describe the complexity of the treatment for a patient based on measurements taken from standard pretreatment orthodontic records, including dental models and cephalometric and panoramic radiographs. In a recent survey looking at the future plans of orthodontic residents, 92.75% planned to use a digital imaging program, and 81.16% planned to become certified by the ABO. Thus, a digital analysis that is accurate and reliable will ease the demonstration of initial case complexity.
Digital models were introduced commercially in 1999 by OrthoCAD (Cadent, Carlstadt, NJ). The results from a recent survey conducted by the Journal of Clinical Orthodontics demonstrate a significant increase in the use of digital diagnostic records from 11% in 1981 to 86.1% in 2013. Today, many companies offer digital models as a replacement for plaster models. Storage of the digital models also varies from company to company. OrthoCAD results in a relatively large file of 3000 kB and in a proprietary format. Motion View Software (Hixson, Tenn) introduced the Ortho Insight 3D scanner and software that use a robotic scanner to produce 3D renderings of impressions or plaster models. The advantage of this software is the flexible, open format of the file produced.
Despite its initial purpose for determining case complexity when selecting cases in preparation for the ABO clinical examination, the use of the DI has also been evaluated for predicting treatment duration. Patients who receive accurate information about treatment duration were found to be more satisfied with their treatment and had more realistic expectations. Thus, the use of DI scores to more accurately predict treatment length may be advocated.
Several studies in the literature have verified the accuracy of linear measurements on 3D digital models with different softwares and found divergent results. A recent systematic review evaluated studies assessing the validity of 7 digital model systems (OrthoCAD, emodel, C3D-builder, ConoProbe, Easy3D Scan, Digimodels, Cecile). The authors concluded that in most studies, the mean discrepancies between plaster and digital model measurements were low. They also noted that based on the variable quality of the available evidence, digital models may be an alternative to plaster models. Recently, a study evaluated the accuracy of Ortho Insight 3D software for assessing tooth width, arch width, and arch length. The authors concluded that 90% of the mean differences were less than 0.20 mm.
The null hypothesis of this study was that there is no statistically significant difference in total DI scores obtained digitally by OrthoCAD or Ortho Insight 3D when compared with total scores obtained by manual measurements made on a plaster model.
Material and methods
In this study, we evaluated manual and digital DI scores obtained from models of varying degrees of complexity. OrthoCAD was chosen based on its popularity in the literature, and Ortho Insight 3D was chosen because of its unique, almost fully automated DI module. Table I lists the key differences between the methods used to calculate the DI scores. The Office for the Protection of Research Subjects of the University of Illinois at Chicago determined in January 2013 that this study (protocol 2013-0090) did not meet the definition of human subject research; therefore, permission to conduct research without further submission to the institutional review board was granted.
| Method | Model | Landmark identification | Scoring |
|---|---|---|---|
| Manual | Plaster | Manually detected by user | Manual calculation |
| OrthoCAD | Digital (obtained from alginate impression) | Digital points detected by user | Points calculated digitally following required user input for tooth selections, contact points, crossbite presence, and molar relationship |
| Ortho Insight 3D | Digital (obtained from scanning plaster model) | Digital points detected by computer and modified by user | No user input |
We assessed 45 pretreatment plaster study models, with 15 models in each category stipulated by the case report category specifications of the ABO’s clinical examination guide to ensure a wide variety of complexities: (1) a DI score less than 10 (would not qualify for use in examination), (2) a DI score greater than 10 but less than 20, and (3) a DI score greater than 20. Study models were assessed for selection criteria and subsequently scored by the primary investigator (K.D.) until 15 sets of models fit into each category according to the DI score while meeting the inclusion and exclusion criteria. The inclusion criteria were pretreatment models trimmed so that when placed on their heels, the teeth occluded in centric occlusion. The exclusion criteria required no supernumeraries, missing teeth (except third molars), deciduous teeth, appliances, fractures, voids, or positive bubbles of plaster.
Calculations of the DI scores manually were obtained by following the instructions of the ABO’s clinical examination guide. Cephalometric parameters were not included in the total DI scores in this study. All raw data measurements were entered into Microsoft Excel for Mac 2011 (version 14.2.3; Microsoft, Redmond, Wash). In addition to point values awarded by target disorders, overjet, overbite, and crowding were recorded in millimeters rounded to the nearest 0.5 mm for the manual measurements and to the nearest 0.1 mm for OrthoCAD and Ortho Insight 3D. For all other target disorders, only point values were collected. Manual measurements were completed on the original plaster casts with a periodontal probe marked in millimeters.
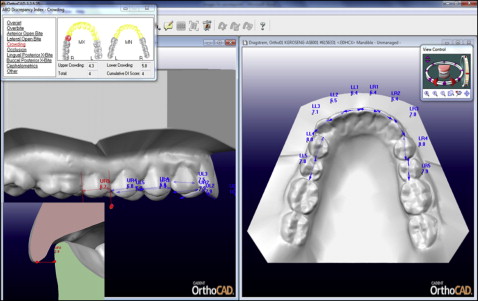
Alginate impressions (Kromopan 100; Kromopan USA, Des Plaines, Ill) and a wax bite registration were taken of each set of plaster models using plastic trays, wrapped in moist towels, sealed in plastic bags, and stored in individual boxes at 37°F overnight until they were sent the next day to OrthoCAD for digitization. OrthoCAD returned the digital 3D models 1 week later to be viewed and manipulated with the proprietary OrthoCAD software (version 3.4; Cadent). The models were visually verified for accuracy of occlusion and, if necessary, were manipulated using the jaw alignment function. OrthoCAD’s ABO DI module computes points and total scores based on user-detected interproximal contacts, arch forms, overbite and overjet measurements, occlusal relationships, buccal and lingual crossbites, diastemas, and spacing ( Fig 1 ). The 3D models were manipulated through zoom or rotation at the examiner’s discretion. When determining tooth widths for measurements of crowding, all 3 planes were verified. Teeth for the evaluations of overjet, negative overjet, overbite, and open bite were selected by the examiner and visually determined for buccal and lingual crossbites and molar relationships.
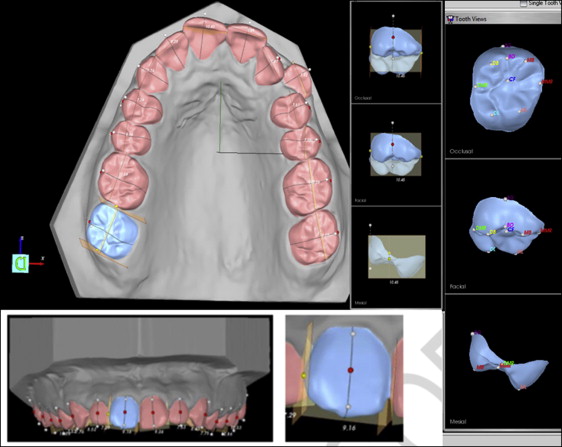
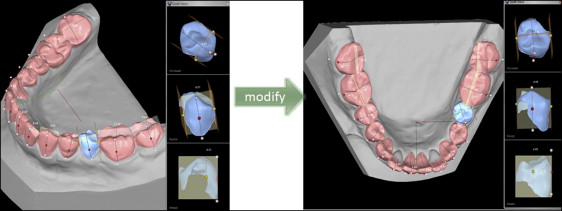
The same plaster models were then scanned by the primary investigator using the Ortho Insight 3D scanner at the slowest speed (for greatest detail capture) and uploaded to the Ortho Insight 3D software (version 4.0.6; Motion View Software). Because the plaster models were already trimmed so that when placed on their heels, the teeth occlude in maximum intercuspation, the software will automatically detect occlusion when the “auto-align” function is chosen. Once the examiner selects all the teeth to be analyzed, the Ortho Insight 3D software will automatically detect occlusal landmarks, interproximal contacts, and long axes of the teeth for DI calculation and appropriately apply points to provide a total DI score ( Fig 2 ). Per Motion View’s recommendation, the examiner reviewed automatically detected occlusal landmarks, interproximal contacts, and long axes, and manually manipulated each point for improved accuracy ( Fig 3 ).
Fifteen casts were selected at random for tests of reliability. Intrarater reliability was completed by the primary investigator by measuring the plaster models for all target disorders and summing the points awarded for the total DI scores twice, separated by a 1-week interval. Digital models corresponding to the same 15 casts were measured and scored twice by the primary investigator using the OrthoCAD software and the Ortho Insight 3D software. Interrater reliability was achieved with a second examiner (J.E.G.). The same 15 casts were sent to the second examiner, who measured for all target disorders and computed the total DI scores. The OrthoCAD files were sent to the second examiner with the ABO’s clinical examination guide for clarification of target disorder definitions. Due to the semiautomated nature of Ortho Insight 3D, interrater reliability was not assessed.
After the reliability testing, the primary investigator measured 45 sets of the initial study models manually, digitally with the OrthoCAD software, and digitally with the Ortho Insight 3D software according to the same guidelines as described in the initial reliability testing. The accuracy of the digital DI scores and its target disorders were compared with the manual scores from the plaster casts.
Statistical analysis
The statistical analysis was conducted with Statistical Package for the Social Sciences (SPSS) software (version 20; IBM, Armonk, NY). Inspection of the raw data set with Shapiro-Wilk tests of normality showed that nonparametric tests were more appropriate to analyze the data because of the nonnormal distribution of all variables. A Spearman rho ( r ) correlation was computed to assess test-retest reliability for all the variables involved in this study. Wilcoxon signed ranks tests were used to test the differences between the mean ranks of the total DI scores and its target disorder scores obtained manually, digitally with OrthoCAD, and digitally with Ortho Insight 3D.
Results
The results for intrarater reliability of the primary investigator assessed with the Spearman rho correlation showed repeated measurements with excellent agreement ( r > 0.8) for all manual measurements except for the category of edge-to-edge open bite ( r = 0.535); for all OrthoCAD measurements except for buccal crossbite, spacing, and diastema (range of correlation, r = 0.608-0.681); and for all Ortho Insight 3D measurements except for left occlusal relationship ( r = 0.775).
The 2 sets of measurements made by the 2 independent examiners on the plaster models were found to be significantly correlated ( r > 0.8), except for the measurements of overjet (points), overbite (points), edge-to-edge open bite, and right occlusal relationship (range of correlation, r = 0.608-0.762); they also had a low correlation for spacing ( r = 0.221). The 2 sets of measurements made by the independent examiners on the OrthoCAD digital models were found to be significantly correlated ( r > 0.8) in all categories except for left occlusal relationship and diastema ( r = 0.763 and 0.535, respectively). Furthermore, all 3 methods demonstrated significantly high intrarater and interrater reliabilities ( r > 0.9) with respect to the total DI score, despite mild to low correlations in a few categories.
The results of the Wilcoxon signed ranks test are shown in Table II . For the purpose of clinical relevance, the descriptive statistics were examined to depict how statistically significant disorders (determined by Wilcoxon signed ranks test) differed between manual calculations, Ortho Insight 3D, and OrthoCAD ( Table III ). Ortho Insight 3D measurements were greater than all manual and OrthoCAD measurements except in the category of spacing. OrthoCAD significantly differed from manual in only overjet (points) and overbite (millimeters) ( Table IV ). According to the descriptive statistics, OrthoCAD overjet was 0.33 points greater than the manual overjet, and the OrthoCAD overbite was 0.62 mm smaller than the manual overbite.


