Orthodontic appliances that become dislodged can cause problems in the airway or the gastrointestinal tract. Accidental ingestion of an appliance during a chair-side procedure or because of inadequate retention of the appliance can create a medical emergency with potentially serious complications, including death from aspiration of the foreign body. This article reports the accidental ingestion of a fractured Twin-block appliance. The ease with which removable appliances can become dislodged if retention is inadequate is discussed, and some serious complications that can arise are described. Precautions the orthodontist can take to prevent such accidents are presented.
Orthodontic appliances or parts of orthodontic appliances can cause problems in the airway or the gastrointestinal tract. Accidental ingestion of an appliance during a chair-side procedure or later, because of inadequate retention of the appliance, can create a medical emergency that can lead to serious complications, including death from aspiration of the foreign body.
The incidence of aspiration or swallowing dental foreign bodies varies considerably in the literature. Tamura et al, in a review article, reported that the range was 3.6% to 27.7% of all foreign bodies, with the number considerably higher in adults than in children. The aspiration or ingestion of orthodontic appliances is less common but no less varied in the types of appliance involved. These include swallowing an expansion appliance key, a transpalatal arch, a lower spring retainer, a fragment of a maxillary removable appliance, and a piece of archwire.
Case report
A 12-year-old boy sought treatment with the chief complaint of pain in the auricular region during wide opening of the mouth for 2 months. On clinical examination, he had tenderness of the masticatory muscles and clicking of the temporomandibular joint during mouth opening. The dental findings included features of Angle Class II Division 1 malocclusion. The cephalometric findings indicated a skeletal Class II malocclusion with a normal maxilla and a retrognathic mandible.
A magnetic resonance image showed an anteriorly displaced articular disc, which was recaptured on mouth opening, confirming the diagnosis of anterior disc displacement with reduction. Treatment was planned to relieve the pain, recapture the anteriorly displaced articular disc, and obtain a skeletal Class I relationship with growth modification. To fulfill the objectives, the patient was given a Twin-block myofunctional appliance. The Twin-block postures the mandible in a forward position until a normal disc-condyle relationship is obtained. It also acts as a splint, brings about disclusion of the teeth, and improves the facial muscle balance.
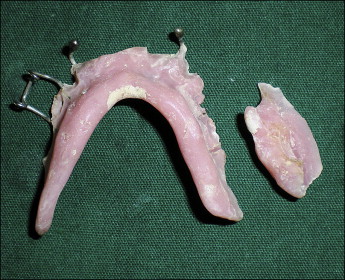
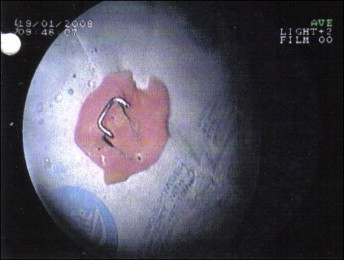
While the patient was using the Twin-block appliance, the lower portion broke after it was dropped ( Fig 1 ). Despite the breakage, he continued to wear the appliance by approximating the broken fragments; he did not report the breakage. While sleeping, he accidentally swallowed a fragment of the appliance; he woke up breathless with a severe cough. The patient moved around, and his father hit him on the back. These efforts to dislodge the obstruction were not effective, and instead it became lodged in the esophagus; this was later confirmed by endoscopy ( Fig 2 ).

The patient was immediately admitted to the hospital, and the broken fragment was removed from the esophagus ( Fig 3 ). He was discharged the same day without further complications.
Discussion
This case report illustrates the ease with which removable appliances can become dislodged if retention is inadequate.
Foreign body ingestion or aspiration has the potential to result in acute medical and life-threatening emergencies. Some complications that can arise are bronchial stenosis, bronchiectasis, lung abcess, tissue ulceration or erosion, esophageal perforation with secondary mediastinitis, pneumothorax, intestinal obstruction, perforation with subsequent abscess formation, and hemorrhage or fistula.
Preventing such incidents via the mandatory use of precautions aimed at securing potentially loose dental objects during all dental procedures is therefore the best approach.
The following precautions should be taken by the orthodontist during the use of removable appliances: (1) all components of removable appliances should be smooth and rounded; (2) hooked or C-clasps should be avoided if possible or alternative retentive components used to reduce the risk of puncturing or irritating the lining of the alimentary canal, and making retrieval without further damage more likely if the appliance becomes impacted; (3) all removable appliances must be suitably retentive and of an adequate size; (4) mandibular removable appliances have a tendency to fracture from the inadequate bulk of the acrylic, especially in the anterior lingual sulcus, so the appliance can be strengthened in this region by incorporation of a rigid wire in the acrylic; (5) the use of different colored acrylic, rather than pink, for removable appliances and retainers has been suggested to avoid the problems of visualizing the acrylic on bronchoscopy or endoscopy if fragments are inhaled or swallowed; and (6) patients should always be advised both verbally and with written instructions at the time of appliance placement that they should not try to reinsert damaged, ill-fitting, or broken fragments of any appliance, and they should stop using them and contact the orthodontist’s office to have the appliance checked.
The orthodontist and the general dentist must be able to recognize signs and symptoms of air obstruction in case a dental object is lost into the oropharynx.
According to the Mayo Clinic website, the universal sign for choking is hands clutched to the throat. If the person does not give the signal, look for these indications: (1) inability to talk; (2) difficulty breathing or noisy breathing; (3) inability to cough forcefully; (4) skin, lips, and nails turning blue or dusky; and (5) loss of consciousness.
If retrieval is not possible, emergency life support measures must be initiated while waiting for help to arrive. If the airway is not compromised, the patient must be escorted to the hospital for clinical and radiographic examinations to identify the location of the object. Treatment thereafter will depend on the findings of the examination.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


