Chapter 9
Endodontic materials
Endodontics is the specialty of dentistry that focuses on the management of prevention, diagnosis and treatment of diseases of the dental pulp and periradicular tissues (region around the root of the tooth).
Dental materials have an important role within endodontics. Along with specialised hand and finger instruments, they facilitate capping exposed pulp, cleaning and shaping the root canal, obturating of the root canal and providing a seal after obturation to prevent contamination of the root canal.
Rubber dam should be routinely used during endodontic treatment to provide the most effective moisture control, safety and cross-infection control.
PULP CAPPING
Pulp capping is a procedure that aims to protect the dental pulp and allows for self-repair of the pulpal exposure. Pulpal exposure occurs most often as a result of trauma, tooth wear, dental caries or accidental exposure during a restorative procedure. Direct pulp capping refers to the procedure of placing a dental material (most often calcium hydroxide) directly over the exposed (or nearly exposed) dental pulp to stimulate reparative or irregular secondary (tertiary) dentine. Indirect pulp capping is the procedure of leaving a thin layer of demineralised dentine over the pulp and placing a dental material (most often calcium hydroxide) over this layer. Removing the source of infection, leaving a small amount of demineralised uninfected dentine and adding calcium hydroxide can encourage the re-mineralisation of the remaining dentine and avoid the risk of pulpal exposure by removing the thin layer of demineralised dentine. Calcium hydroxide is used for pulp capping because of its antibacterial properties and its ability to stimulate the formation of irregular secondary (tertiary) dentine. Mineral Trioxide Aggregate is also indicated for this use (see p. 145).
CALCIUM HYDROXIDE
Calcium hydroxide is a dental liner (see Chapter 7) that stimulates the formation of irregular secondary (tertiary) dentine. It will be discussed in this chapter as a pulp capping material .
Material constituents/composition
Most often supplied in a two-paste system – ‘catalyst’ and ‘base’. Constituents vary between manufacturers. The constituents listed below are specific to Life (Kerr, 2006).
| Catalyst | Base |
| Barium sulphate | Calcium hydroxide |
| Titanium dioxide | Zinc oxide |
| Methyl salicylate | Butyl benzene solfonamide |
Calcium hydroxide is the active ingredient in the material, and the other ingredients may vary depending on the manufacturer.
Calcium hydroxide may also be supplied in a light-cured form:
| Light-cured form |
| Urethane dimethacrylate resin |
| Calcium hydroxide |
| Barium sulphate fillers |
Properties
- Low thermal conductivity
- Stimulates the production of irregular secondary (tertiary) dentine
- pH of 11–12 (i.e. alkaline)
- Bactericidal
- Highly soluble (with the exception of the visible light-cured form)
Advantages
- Easily manipulated
- Stimulates the formation of irregular secondary (tertiary) dentine
Disadvantages
- Moisture sensitive
- Low strength
- Opaque
- Very soluble
Indications and contraindications for use
Indications
- For use with direct or indirect pulp capping within 2 mm of pulp
- For use under permanent restorative materials
- Used in the deepest portion of cavity preparation
- May be used underneath a base
Contraindications
- Cannot be applied in a thick layer
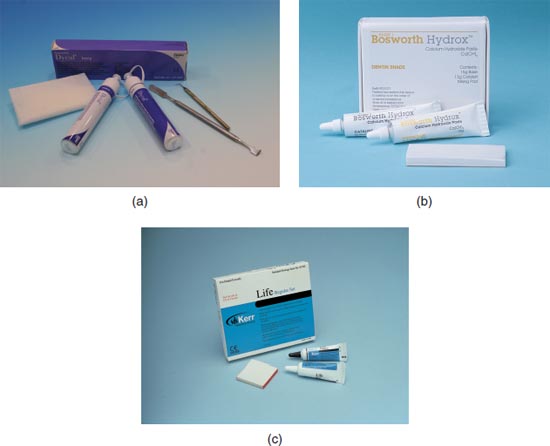
Trade names
| Trade name | Manufacturer |
| Dycal® (Figure 9.1a) | Dentsply |
| HydroxTM (Figure 9.1b) | Bosworth |
| Life (Figure 9.1c) | Kerr |
| VLC Dycal® | Dentsply |
Figure 9.1 (a) Dycal® – Dentsply. (b) HydroxTM – Bosworth. (c) Life – Kerr.
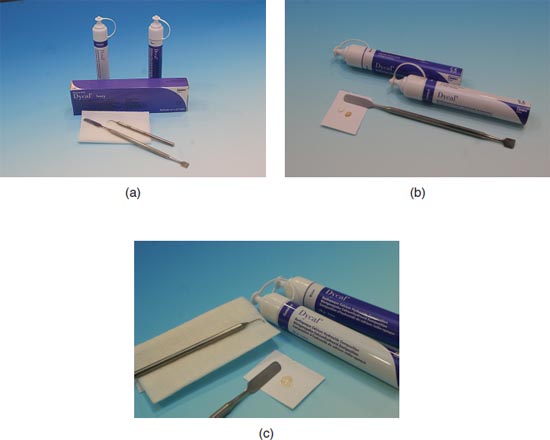
Manipulation (Figures 9.2a–9.2c)
Wearing personal protective equipment:
Two-paste system:
- Dispense equal volume of both catalyst and base onto a waxed paper pad according to the manufacturer’s instructions (use sparingly as not much material is needed)
- Do not allow the two pastes to touch as this will prematurely initiate the setting reaction
- Ensure that the correct caps are replaced on the appropriate tube to prevent cross-contamination of the base and catalyst
- Mix pastes together in a circular motion until a homogeneous colour is achieved (10–15 seconds)
- Pass the material to the operator along with a calcium hydroxide applicator for application
- Have some gauze at hand to wipe the calcium hydroxide applicator in between applications
- Receive the calcium hydroxide applicator from the operator
- Wipe any excess material from the spatula
- Dispose of the paper mixing pad in the contaminated waste bin
Light-cured system:
- Dispense material or attach new syringe tip
- Pass the material to the operator with a calcium hydroxide applicator for application, or pass syringe
- Have some gauze at hand to wipe instrument in between applications
- Receive the calcium hydroxide applicator from the operator
- Light cure the calcium hydroxide and extend the amber light protection shield to protect the eyes of the operator and assistant
- Wipe excess material from the calcium hydroxide applicator
- Dispose of the syringe tip and or waxed paper pad in the contaminated waste
- Two-paste system – 10 to 15 seconds, light cured and no mixing required
- Two-paste system – 1.5 to 2.5 minutes, light-curing material – immediately upon polymerisation
Instruments and materials used in set-up
- Calcium hydroxide material
- Waxed paper pad
- Mixing spatula
- Calcium hydroxide applicator
- Gauze
For light curing:
- Curing light
- Amber light protection shield
Figure 9.2 (a) Calcium hydroxide set-up. (b) Calcium hydroxide dispensed. (c) Calcium hydroxide homogenous mix.
MINERAL TRIOXIDE AGGREGATE
Mineral Trioxide Aggregate (MTA) is an endodontic cement that is biocompatible and hydrophilic. It is a powder that is mixed with distilled water.
Material constituents/composition
- Tricalcium oxide
- Silicate oxide
- Bismute oxide
Properties
- Sets in a wet environment
- Setting time is 3–4 hours
- Often referred to as the ‘gold standard’
- Placed in oral cavity with an amalgam carrier
Advantages
- Biocompatible
- Antimicrobial
- Hydrophilic properties
- Sealing properties
- Radiopaque
Disadvantages
- Expensive
- Difficult manipulation
- Powder sensitive to humidity – the cap must be replaced immediately after dispensing
Indications for use
Indications
- Sealant in endodontics (perforation of root canal)
- Apexification (non-surgical root canal treatment)
- Repair of root perforations during endodontics
- Direct pulp capping
- Pulpotomy
- Apexogenesis (non-surgical root canal treatment)
Trade names
| Trade name | Manufacturer |
| ProRoot | Dentsply |
Manipulation (Figures 9.3a–9.3c)
Wearing personal protective equipment:
- Dispense one scoop of MTA and one drop of distilled water on glass slab
- Ensure cap of powder is replaced immediately after dispensing as it is sensitive to humidity
- Mix powder and water together with a Weston spatula until a homogenous mixture is achieved (mixing time is 30 seconds)
- The final mixture should resemble wet sand
- Fill amalgam carrier and pass to operator to condense in desired location
- Clean and disinfect surface and dispose of excess material in the contaminated waste bin
- 30 seconds
- Initial: 10 minutes; Final: 15 minutes
Figure 9.3 (a) MTA set-up. (b) MTA dispensed. (c) MTA mixed.
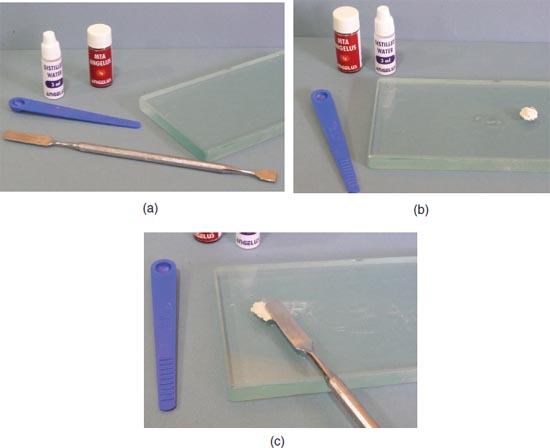
Instruments and materials used in set-up
- MTA material
- Glass slab
- Weston spatula
- Amalgam carrier
- Dappen dish
IRRIGANTS AND LUBRICANTS
Irrigants and lubricants are used during endodontic treatment to flush and disturb debris from the root canal, for disinfection of the root canal, and other functions. A variety of lubricants and irrigations are used. The operator should choose a solution that is an effective, non-toxic lubricant and which has the ability to flush and break down organic debris from the canal and disinfect it. A disposable blunt-needle syringe is used to deliver the irrigant to the root canal. The dental nurse must always use the high-volume suction during canal irrigation.
Material constituents/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


