CHAPTER 9
Dry mouth, excess salivation, coated tongue, halitosis, and altered taste
• Excess salivation (sialorrhea)

General approach
• Although the presence of xerostomia or excess salivation can usually be determined easily, the successful management of these conditions involves a range of clinical and special investigations to determine the underlying cause.
• The tongue has a natural degree of white coating in health. However, this coating can become excessive or undergo color change.
• Bad breath (halitosis) or altered taste is a frequent complaint. This usually represents an oral hygiene problem but an underlying disease should not be excluded if a local cause cannot be found.
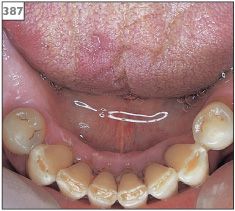
387 Saliva pooling in the floor of the mouth.
Excess salivation (sialorrhea)
ETIOLOGY AND PATHOGENESIS
Baseline production of saliva is often increased in a patient who has oral ulceration or is wearing a new denture for the first time. In such circumstances, stimulation of the salivary glands resolves once the ulceration heals or the oral tissues adapt to the new denture. Certain neuromuscular disorders, in particular Parkinson’s disease and cerebral palsy, limit the ability to swallow and can result in apparent excess saliva.
CLINICAL FEATURES
There may be obvious pooling of saliva in the floor of the mouth (387) and drooling. However, it is not uncommon for patients to complain of excessive salivation, but no clinical abnormality is present.
DIAGNOSIS
There are no specific tests to confirm the presence of excess salivation. The diagnosis is made on clinical observation alone.
MANAGEMENT
Application of a self-adhesive hyoscine (scopolamine) patch every 72 hours has been reported to be helpful in reducing saliva production in some patients. Surgical redirection of excretory ducts of the major salivary glands into the posterior oropharnyx can be also be considered. If clinical examination reveals no evidence of excess saliva, then a psychological assessment should be arranged.
Xerostomia (dry mouth)
ETIOLOGY AND PATHOGENESIS
A reduced production of saliva is usually due to one of the following: an adverse effect of drug therapy, an immune-related disease, radiation damage, or dehydration. Anxiety may also limit the production of saliva, both on an acute or a chronic basis. Xerostomia due to congenital abnormalities or development failure of the salivary glands is extremely rare.
CLINICAL FEATURES
The clinical presentation of xerostomia or reduced salivary production is the same, regardless of the cause. Patients complain of a number of symptoms, in particular difficulty in talking or swallowing, altered taste, generalized oral discomfort, and, if worn, poor retention of dentures. A reduction in saliva flow of greater than 50% is usually required before clinical symptoms develop. Examination will reveal a lack of saliva in the floor of the mouth and attempts to express saliva from the major salivary duct openings by external pressure on the gland may fail. In addition to being reduced in amount, any saliva that is present may be frothy in nature (388). The buccal mucosa becomes sticky and will adhere to the face of a dental mirror placed against it. Lack of saliva will produce a generalized erythema of the oral mucosa (389, 390) and a lobulated appearance on the dorsum of the tongue (391). There is also likely to be evidence of candidosis (candidiasis) and angular cheilitis. The teeth are prone to cervical caries and existing restorations may fail due to recurrent caries (392–395). Patients with xerostomia are also predisposed to recurrent episodes of bacterial sialadenitis, particularly of the parotid gland (Chapter 6, p. 116).


389 Erythematous and atrophic mucosa due to xerostomia.

390 Erythematous and atrophic mucosa due to xerostomia.

391 Lobulated tongue due to xerostomia.
DIAGNOSIS
Xerostomia can be diagnosed clinically on the basis of little or no saliva pooling in the floor of the mouth at rest. Unfortunately, determination of the underlying cause of xerostomia may be problematic and requires a range of special investigations. The patient’s medical history may reveal the possibility of drug-induced xerostomia, particularly if the onset of symptoms coincided with the provision of a new medication. Drugs that are known to produce xerostomia include antidepressants, antihistamines, anticholinergi/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


