INTRODUCTION
PURPOSE OF TOOTH PREPARATION
• Preventing and Treating Caries
• Replacing Restorations
• Treatment of Malformed, Fractured and Traumatized Teeth
• Esthetic Improvement
• For Restoration of Loss of Tooth Material
• Types of Restoration
TERMINOLOGY OF TOOTH PREPARATION
• Tooth Preparation
• Simple, Compound and Complex Tooth Preparation
• Tooth Preparation Walls
• Cavosurface Angle Margin/Tooth Preparation Margin
• Angle
NUMBER OF LINE ANGLES AND POINT ANGLES IN DIFFERENT TOOTH PREPARATION DESIGNS
• Class I Tooth Preparation
• Class II Tooth Preparation
• Class III Tooth Preparation
• Class IV Tooth Preparation
• Class V Tooth Preparation
TOOTH PREPARATION
• Classification of Tooth Preparations
STEPS IN TOOTH PREPARATION
• Initial Tooth Preparation
• Final Stages of Tooth Preparation
• Air Abrasion/Kinetic Tooth Preparation
• Technique
• Advantages of Air Abrasion
• Disadvantages
• Uses of Air Abrasion Technology
INTRODUCTION
Operative dentistry requires essential knowledge of basic tooth preparation, which is important to the dental practitioner. The most important fundamental procedure of operative dentistry is tooth preparation to receive a restoration so that it can fulfill all its requirements. There-fore, it is a must for every operative clinician to be well aware of all the fundamentals of the tooth preparation. A cavity is a defect in the mineralized dental tissues which results from pathological processes like caries, attrition, abrasion and erosion.
The tooth preparation includes all mechanical procedures performed to remove all infected and affected tissues and to give proper design to the remaining hard dental tissues, so that a mechanically and biologically sound restoration can stay in the prepared tooth. Tooth preparation is a surgical procedure that removes the caries till the sound tooth tissue of proper shape is reached which will retain a restorative material that resists masticatory forces, maintains form function and esthetics.
PURPOSE OF TOOTH PREPARATION
Restoration is usually required to repair a diseased, injured or defective tooth structure. The restoration helps in maintaining proper form, function and esthetics.
Preventing and Treating Caries
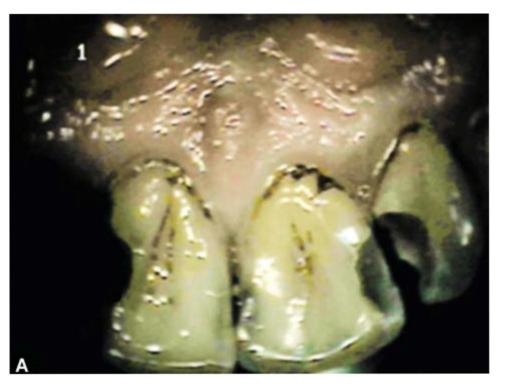
Dental caries is one of the most common diseases with approximately 80% of the population in developed countries (Fig. 7.1).
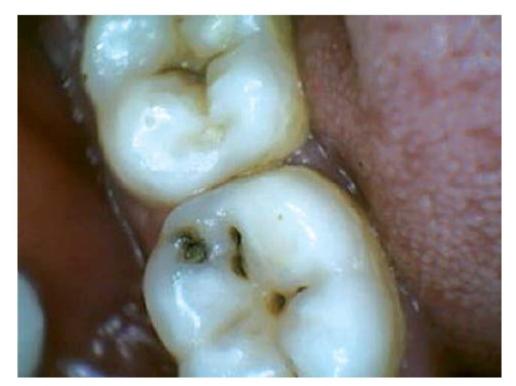
Fig. 7.1: Photograph showing carious tooth which needs restoration
The aim of prevention and treatment is to maintain a functioning set of teeth. Interventions can halt and even reverse the development of caries.
Replacing Restorations
Restorations may fail due to a number of “objective” factors which further depend upon characteristics of the restorative material, operator skill and technique, patients’ dental characteristics, and the environment around the tooth.
The decision to replace a restoration is affected by factors such as condition of restoration, health of the tooth, and the criteria used to define failure and patient demand (Fig. 7.2).

Fig. 7.2: Photograph showing an old restoration needing replacement
Treatment of Malformed, Fractured and Traumatized Teeth
Restorations are needed to treat malformed, fractured or traumatized teeth so as to retain them to normal form and function.
Esthetic Improvement
Teeth which are unesthetic and discolored can be treated by esthetic restorations.
For Restoration of Loss of Tooth Material
Attrition, abrasion or erosion of teeth can be treated by different restorative materials depending upon the extend and location of the lesion.
Types of Restoration (Figs 7.3A and B)
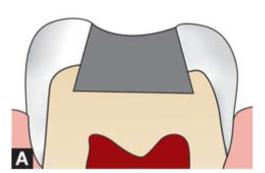
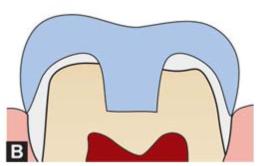
Figs 7.3A and B: (A) Intracoronal amalgam restoration, (B) Extracoronal restoration
Tooth restoration may be classified as intracoronal, when it is placed within a preparation made in the crown of a tooth or extracoronal, when it is placed outside the tooth as in the case of a crown. Intracoronal restoration is placed directly into the tooth preparation while extracoronal restoration uses an indirect technique.
The materials used to restore teeth are: dental amalgam, composite resins, glass ionomer cements, resin-modified glass ionomer cements, compomers and cermets, cast gold and other alloys, and porcelain.
Factors affecting the decision to restore a tooth
Tooth factors
• Primary or permanent
• Occlusal stresses
• Quality of tooth (hypoplasia)
• Location of tooth
• Type of tooth
• Type of tooth preparation.
General patient factors
• Patient’s exposure to fluoride
• Age
• Xerostomia
• Socioeconomic status
• Diet
• Caries status
• General health
• Presence of any parafunctional habit.
Factors related to clinician and the restoration to be used
• Type of restoration
• Physical properties of the restoration
• Whether moisture control can be achieved or not
• Technical expertise
TERMINOLOGY OF TOOTH PREPARATION
Tooth Preparation
It is a mechanical alteration of a defective, injured or diseased tooth in order to best receive a restorative material which will re-establish the healthy state of the tooth including esthetics correction when indicated along with normal form and function (Fig. 7.4).

Fig. 7.4: Photograph showing tooth preparation on molar
Simple, Compound and Complex Tooth Preparation
Simple Tooth Preparation
A tooth preparation involving only one tooth surface is termed simple preparation (Fig. 7.5). For example, mesial, distal, occlusal, buccal, lingual tooth preparation.
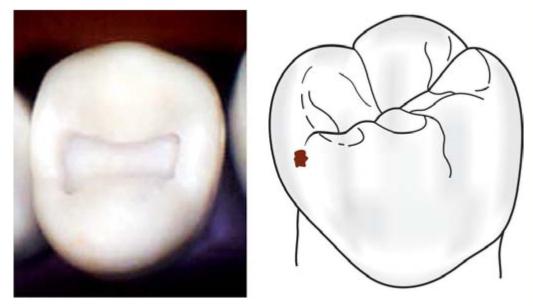
Fig. 7.5: Simple tooth preparation involving one tooth surface only
Compound Tooth Preparation
A tooth preparation involving two surfaces is termed compound tooth preparation (Fig. 7.6). For example, mesio-occlusal (MO), disto-occlusal (DO), mesiolingual (ML), or distobuccal (DB) tooth preparation.
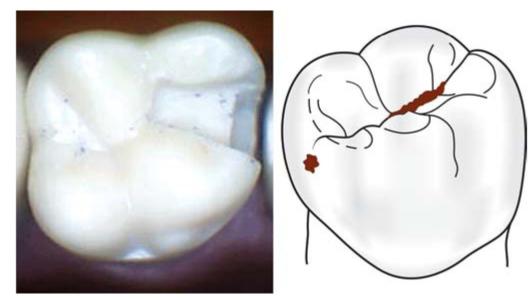
Fig. 7.6: Compound tooth preparation involving two surfaces
Complex Tooth Preparation
A tooth preparation involving more than two surfaces is called as complex tooth preparation (Fig. 7.7). For example, mesio-occlusodistal (MOD), facio-occlusolingual (FOL) or mesioincisodistal (MID) tooth preparation.
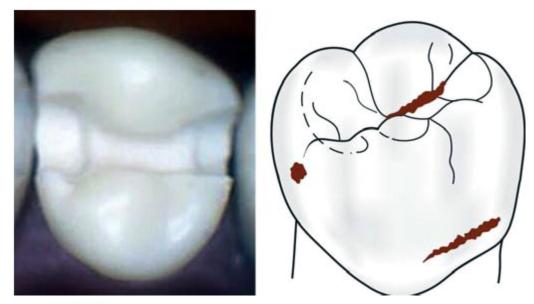
Fig. 7.7: Complex tooth preparation involving more than two surfaces
Tooth Preparation Walls
Wall
Any surface of the tooth preparation is referred to as a wall.
Internal Wall
It is a wall in the preparation, which is not extended to the external tooth surface (Fig. 7.8).
Fig. 7.8: Internal wall of tooth preparation
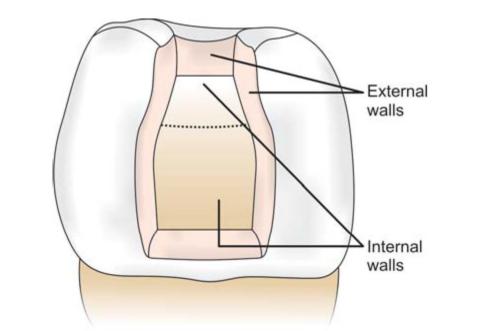
External Wall
An external wall is a wall in the prepared tooth surface that extends to the external tooth surface (Fig. 7.9). External wall takes the name of the tooth surface towards which it is situated.
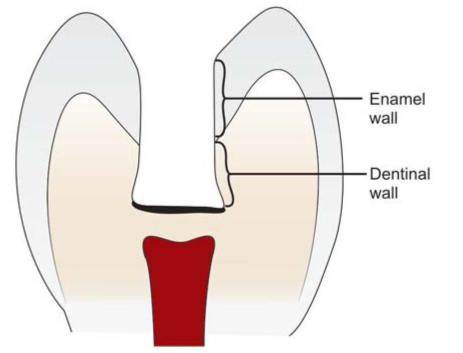
Fig. 7.9: External wall of tooth preparation
Enamel Wall
An enamel wall that portion of tooth preparation which is composed of enamel.
Dentin Wall
A dentin wall that portion of tooth preparation which is composed of dentin.
Dentinoenamel Junction
Dentinoenamel junction is the line representing the junction of enamel and dentin.
Cementoenamel Junction
Cementoenamel junction is the line representing the junction of enamel and dentin.
Pulpal Wall
A pulpal wall is an internal wall that is towards the pulp and covering the pulp (Fig. 7.10). It may be both vertical and perpendicular to the long axis of tooth.
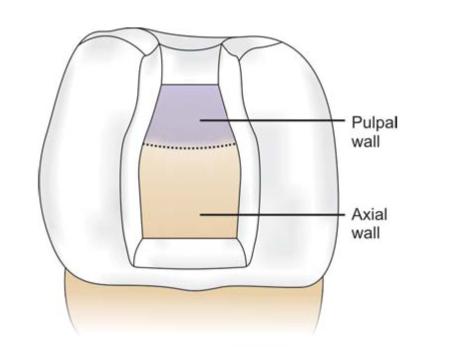
Fig. 7.10: Pulpal wall
Axial Wall
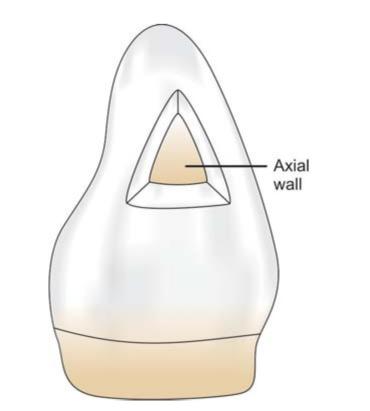
Fig. 7.11: Axial wall
It is an internal wall which is parallel to the long axis of the tooth (Fig. 7.11).
Step
It is an auxiliary extension of the main tooth preparation on to an adjoining surface. For example in class III tooth preparation with lingual dovetail is called as lingual step.
Floor
Floor is a prepared wall which is usually flat and perpendicular to the occlusal forces directed occlusogingivally, for example, pulpal and gingival walls (Fig. 7.12).
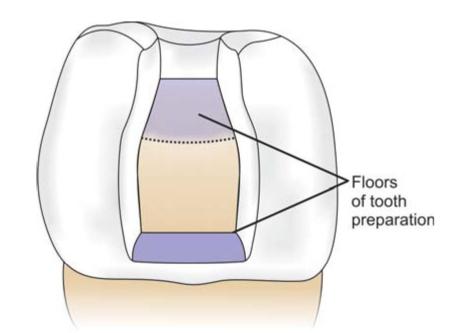
Fig. 7.12: Pulpal and gingival floors of a class V tooth preparation
Cavosurface Angle Margin/Tooth Preparation Margin
Cavosurface angle is formed by the junction of a prepared tooth surface wall and external surface of the tooth (Fig. 7.13). The acute junction is referred to as preparation margin or cavosurface margin. The cavosurface angle may differ with the location of tooth and enamel rod direction of the prepared walls and also differ according to the type of restorative material to be used (Figs 7.14 and 7.15).
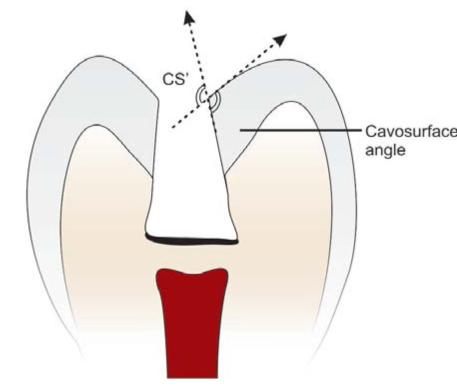
Fig. 7.13: Cavosurface margin
Fig. 7.14: Butt joint cavosurface margin for amalgam
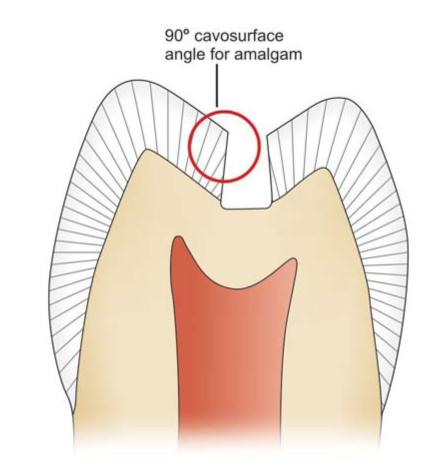
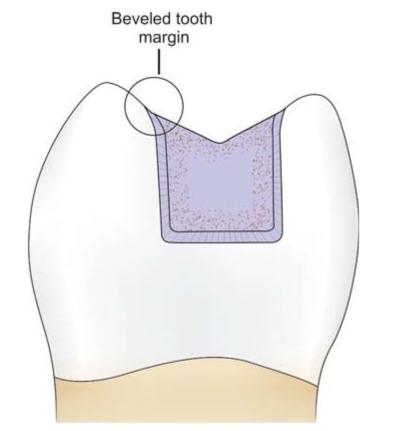
Fig. 7.15: Beveled cavosurface margin for cast gold restoration
Angle
A junction of two or more surfaces of tooth preparation is termed as an angle.
Line Angle
It is a junction of two surfaces of different orientations along the line and its name is derived from the involved surfaces.
Point Angle
It is a junction of three plane surfaces or three line angles of different orientation and its name is derived from its involved surfaces or line angles.
Pulpal Line Angle
Any angle perpendicular to long axis of tooth is called pulpal line angle.
Axial Line Angle
Any angle parallel to long axis of tooth is called axial line angle.
How to Combine Different terms?
When one word is to be formed by combination of two or more walls or surfaces, the “al” word of prefix word is replaced with “0”. For example, if distal and occlusal words are to be combined, the combined term will be distocclusal. The combined word of mesial, distal and occlusal surface is mesio-occlusodistal.
NUMBER OF LINE ANGLES AND POINT ANGLES IN DIFFERENT TOOTH PREPARATION DESIGNS
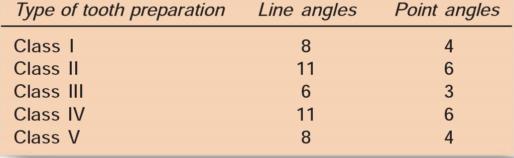
The line angles and point angles of different tooth preparation designs are as follows:
Number of line angles and point angles in different tooth preparation designs
Class I Tooth Preparation
For simple class I tooth preparation involving only occlusal surface of molars eight line angles and four-point angles are named as follows (Fig.7.16):
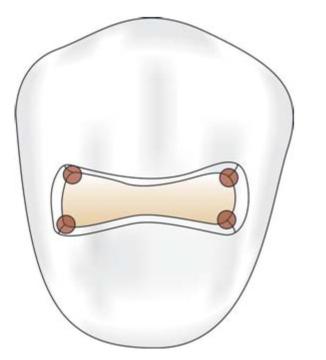
Fig. 7.16: Class I tooth preparation showing line angle and point angles
Line Angles
• Mesiobuccal line angle
• Mesiolingual line angle
• Distobuccal line angle
0 Distolingual line angle
• Faciopulpal line angle
• Linguopulpal line angle
• Mesiopulpal line angle
• Distopulpal line angle.
Point Angles
• Mesiobuccopulpal point angle
• Mesiolinguopulpal point angle
• Distobuccopulpal point angle
• Distolinguopulpal point angle.
Class II Tooth Preparation
For class II preparation (mesio-occlusal or disto-occlusal) 11 line angles and 6-point angles are as follows (Fig. 7.17). The following is the nomenclature for mesio-occlusal tooth preparation.
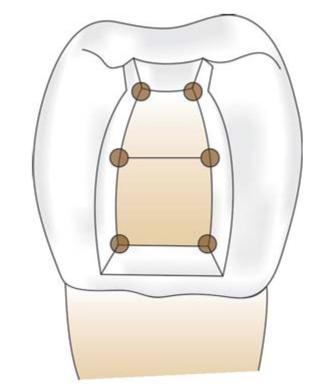
Fig. 7.17: Class II tooth preparation showing line and point angles
Line Angles
• Distofacial
• Faciopulpal
• Axiofacial
• Faciogingival
• Axiogingival
• Linguogingival
• Axiolingual
• Axiopulpal
• Distolingual
• Distopulpal
• Linguopulpal
Point Angles
• Distofaciopulpal point angle
• Axiofaciopulpal point angle
• Axiofaciogingival point angle
• Axiolinguogingival point angle
• Axiolinguopulpal point angle
• Distolinguopulpal point angle.
Class III Tooth Preparation
For class III preparation on anterior teeth 6 line angles and 3-point angles are as follows (Fig. 7.18).
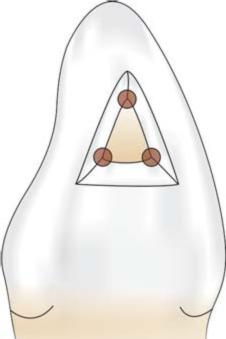
Fig. 7.18: Class III preparation showing line and point angles
Line Angles
• Faciogingival
• Linguogingival
• Axiogingival
• Axiolingual
• Axioincisal
• Axiofacial
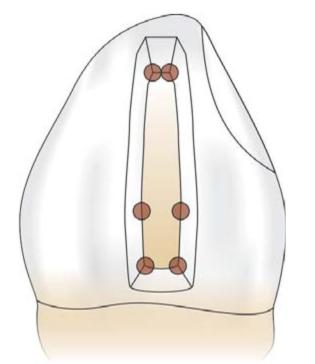
Fig. 7.19: Class IV preparation showing line and point angles
Point Angles
• Axiofaciogingival point angle
• Axiolinguogingival point angle
• Axioincisal point angle.
Class IV Tooth Preparation
For class IV tooth preparation on anterior teeth, 11 line angles and 6-point angles are as follows (Fig. 7.19).
Line Angles
• Faciogingival
• Linguogingival
• Mesiofacial
• Mesiolingual
• Mesiopulpal
• Faciopulpal
• Linguopulpal
• Axiogingival
• Axiolingual
• Axiofacial
• Axiopulpal.
Point Angles
• Axiofaciopulpal point angle
• Axiolinguopulpal point angle
• Axiofaciogingival point angle
• Axiolinguogingival point angle
• Distofaciopulpal point angle
0 Distolinguopulpal point angle.
Class V Tooth Preparation
For class V preparation, 8 line angles and 4-point angles are as follows (Fig. 7.20).
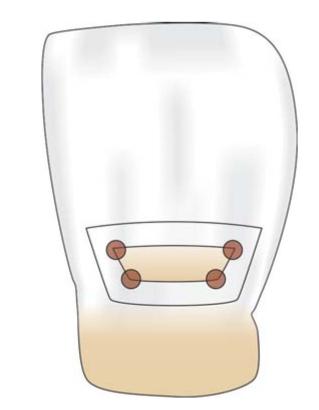
Fig. 7.20: Class V preparation showing line and point angles
Line Angles
• Axiogingival
• Axioincisal
• Axiomesial
• Axiodistal
• Mesioincisal
• Mesiogingival
• Distoincisal
• Distogingival.
Point Angles
• Axiodistogingival point angle
• Axiodistoincisal point angle
• Axiomesiogingival point angle
• Axiomesioincisal point angle.
TOOTH PREPARATION
Black gave following guidelines for tooth preparation:
• Providing definite mechanical retention in the preparation.
• Extension of preparation in adjacent pits and fissures for prevention of recurrent caries.
• Removal of infected and affected dentin from all surfaces.
• Removal of even healthy tooth structure to gain access and good visibility.
When Black gave classification, following conditions and considerations were prevalent at that time:
• Poor oral hygiene habits.
• Poor properties of the existing restorative materials.
• The expected longer life of the restoration.
• Hard and fibrous food.
• Low consumption of refined carbohydrates.
• More liking towards gold and silver fillings in teeth.
• Prevailing common diagnostic aids such as PMT.
Nowadays because of change in following conditions, design of the tooth preparation has become most conservative:
•Use of preventive measures like fluoridation of water supply, fluoride toothpaste, topical fluoride applications, proper brushing and flossing, etc.
• Understanding of the fact that the remineralization of enamel and affected dentin can take place.
• Advances in tooth colored, adhesive, fluoride releasing restorative materials.
• Newer advancements in restorative materials.
• Improvements in diagnostic aids.
• Better oral hygiene maintenance.
• Mechanical retention forms further improve the retention.
Classification of Tooth Preparations
Tooth preparations may be classified according to the location where the carious lesion initiates. Caries oftenly initiate in the developmental pits and fissures of the teeth. These areas are morphologically deeper than the surrounding tooth substance and are thus sites for food impaction and nearly impossible to clean thoroughly, forming ideal conditions for bacterial plaque formation (Fig. 7.21).

Fig. 7.21: Deep pits and fissures are primary areas for food impaction and caries formation
Commonly seen locations of pit and fissure in teeth are:
• Palatal pits of maxillary incisors.
• Palatal grooves and pits of maxillary molars.
• Occlusal surfaces of posterior teeth.
• Facial grooves and pits of mandibular molars.
• Pits occurring in teeth because of irregularities in the enamel formation.
Smooth surface lesions can be found in all teeth on the proximal surfaces, and gingival one-third of the facial and lingual surfaces. GV Black gave a simple classification based on clinical location of the defects, listed as class I, class II, class III, class IV and class V. An additional class VI was later on added by Simon as modification to Black’s classification.
Class I is the only pit and fissure preparation whereas rest are smooth surface preparations.
Class I.• Pit and fissure preparations occur on the occlusal surfaces of premolars and molars, the occlusal two-third of buccal and lingual surface of molars, lingual surface of incisors and any other abnormal position (Figs 7.22A and B).

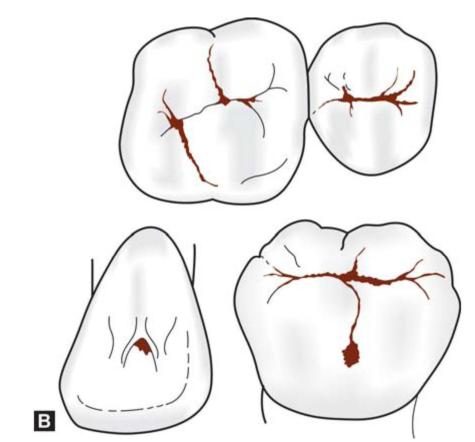
Figs 7.22A and B: (A) Clinical presentation of class I lesion, (B) Diagrammatic presentation of class I lesion
Class IT Preparations on the proximal surface of premolars and molars are class II (Figs 7.23A and B).

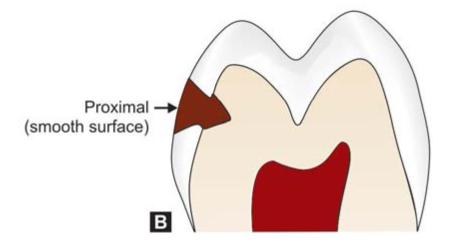
Figs 7.23A and B: (A) Class II lesion, (B) Diagrammatic presentation of class II lesion
Class III: Preparations on the proximal surface of anterior teeth and not involving the incisal angles are class III (Figs 7.24A and B).
Class IV: Preparations on the proximal surface of anterior teeth also involving the incisal angle come under class IV (Figs 7.25A and B).
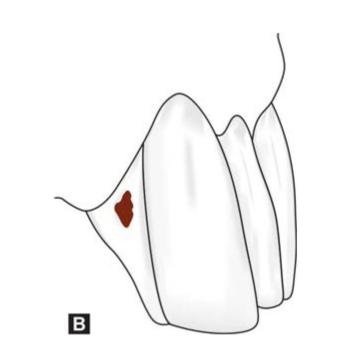
Class V.• Preparations on gingival third of facial and lingual or palatal surfaces of all teeth came under class V (Figs 7.26A and B).
Modification of Black’s classification was made to provide more specific localization of preparations.
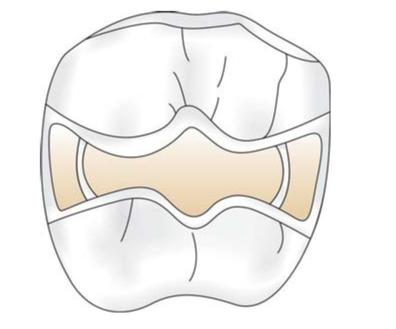
Class IT Preparations on the single or both proximal surface of premolar and molar teeth. When there is involvement of both proximal surfaces, it is called mesio-occlusodistal (MOD) preparation (Fig. 7.27).
Figs 7.24A and B: (A) Class III lesion, (B) Diagrammatic representation of class III lesion


Figs 7.25A and B: (A) Class IV lesion, (B) Diagrammatic representation of class IV defect

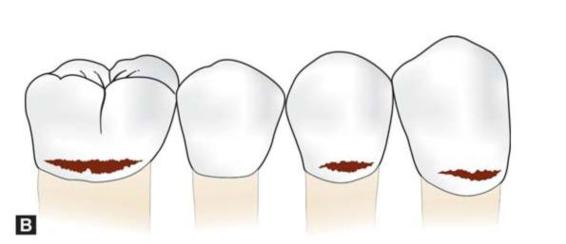
Figs 7.26A and B: (A) Class V lesion, (B) Diagrammatic representation of class V lesion
Fig. 7.27: MOD preparation
Class VI: Preparations on incisal edges of anterior and cusp tips of posterior teeth without involving any other surface (Fig. 7.28) come under class VI.
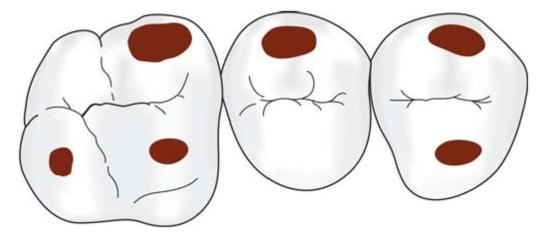
Fig. 7.28: Class VI lesion are present on cuspal tips
STEPS IN TOOTH PREPARATION
Before initiating tooth preparation one should identify presence of caries. There should be an opacity surrounding the pit and fissure indicating demineralization of the enamel. Softened enamel can be detected and removed away with the sharp tip of explorer.
After the clinician decides which tooth to restore, the anesthesia is given.
Tooth preparation involves a systemic approach based on the mechanical and physical principles which should be followed in an orderly sequence. The design of the tooth preparation for either a tooth with initial caries or replacement restoration depends upon location of the caries, the amount and extent of the caries, the amount of lost tooth structure, and the restorative material to be used. But there are some basic principles which should be followed while doing tooth preparation.
Earlier when the affected tooth was prepared because of caries, cutting of tooth was referred to as cavity preparation. But nowadays many indications other than caries lead to preparation of the tooth. Hence, the term cavit/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


