CHAPTER 7 Treatment of the Edentulous Maxilla
Zygoma Implant Concept
Radiographic Evaluation
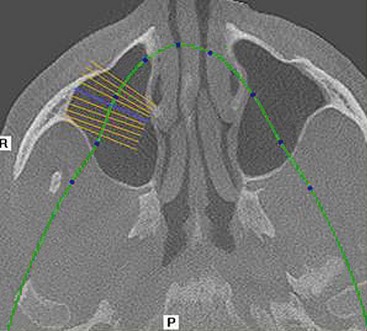
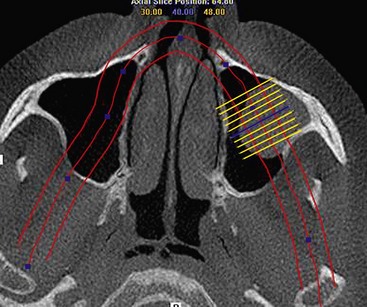
Although computed tomography (CT) or conventional tomography can be used, the panoramic radiograph is critical in initial patient evaluation.1–3 Axial CT scans and cone beam technology can be used to further evaluate the maxillary sinus. The width of the residual alveolar bone and the width and height of the zygomatic body can be visualized in frontal (Figure 7-1) or axial (Figure 7-2) reformatted sections.

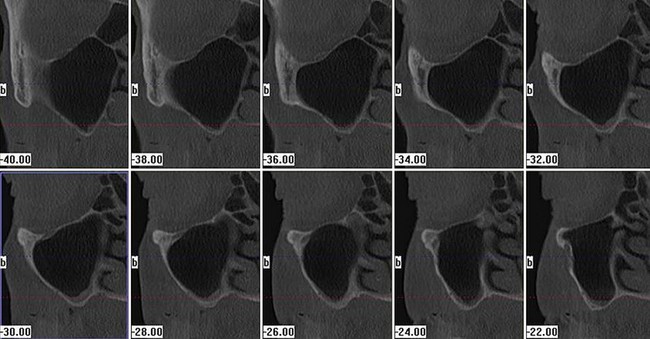
Further evaluation of the zygomatic bone has also been described.4 Although not absolutely necessary, the reformatted frontal images in 0.5- to 1-mm cuts afford the less experienced operator more information for surgery planning (Figure 7-3). Pathologic conditions in the sinus, including but not limited to thickening of the Schneiderian membrane as well as air-fluid levels, may be ruled out in both the panoramic radiographic examination as well as the tomographic studies (Figure 7-4).
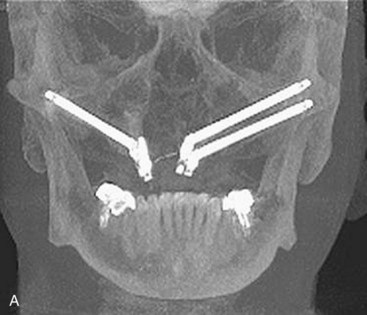
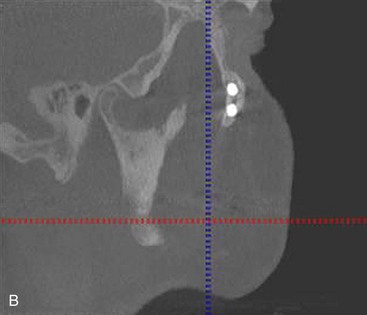
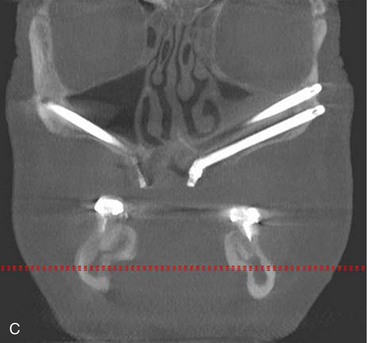
Cone beam CT scan can also be used effectively to manipulate postoperative radiographs (Figure 7-5, A). The ability to manipulate the cone beam images to demonstrate apex positioning of the zygoma implant within the zygoma body (Figure 7-5, B), as well as the relationship of the zygoma implant platform to the crestal portion of the alveolus, leads to a better understanding of surgical technique (Figure 7-5, C).
Preoperative Considerations
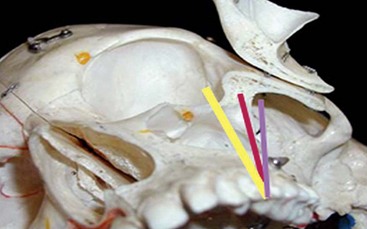
The surgical procedure is usually performed in the office setting under intravenous (IV) sedation,1,5 although the procedure can be performed under local anesthesia or in the operating room under general anesthesia. All patients are premedicated with 2 g of penicillin or 600 mg of clindamycin 1 hour prior to the procedure. Proper administration of sufficient local anesthesia is critical to manage patients under IV sedation. The various infiltrations and nerve blocks include circumvestibular infiltration of the maxilla and greater palatine nerve blocks, as well as bilateral transcutaneous infiltration of the temporal areas over the zygomatic body. Bilateral inferior alveolar nerve blocks are considered to allow retraction of the lower jaw during surgery without undo stimulation of the sedated patient. It is recommended that the path of the implant from the premolar area to the base of the zygoma be directly visualized whenever possible.1,6 Direct visualization of the base of the zygoma body has also been advocated by clinicians who have used computer-assisted treatment planning and surgical templates for placement of zygomatic implants.6 Having a clear view of the instruments’ path while establishing the osteotomy, as well as visualizing the path of the implant during its insertion, avoids disorientation and potential complications. Generally, three potential axes for implant insertion are possible. The proper axis is a path extending from the bicuspid region through the maxillary sinus, entering the mid portion of the zygomatic body. If the entry point in the zygomatic body is anterior to this line axis, potential exists for penetration into the orbit. If the line axis is posterior to this line, potential exists for entering the pterygomaxillary space, which leads to soft tissue envelopment and subsequent lack of osseointegration of the implant, causing unexpected hemorrhage (Figure 7-6).
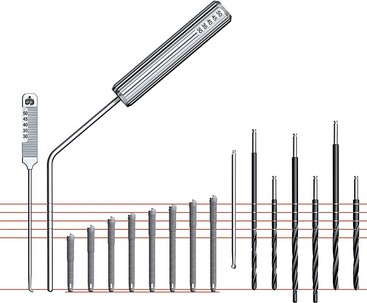
The zygomatic implant has a unique design. The diameter of the apical two-thirds of the implant is 4 mm and the alveolar one-third widens to a diameter of 5 mm. Zygomatic implants are available in lengths ranging from 30 to 52.5 mm. A specialized series of long zygoma drills are used to prepare the osteotomy (Figure 7-7).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


