Chapter 7
Aesthetic Compromises and Dilemmas
Aim
Success is a poor teacher. We learn a great deal from our mistakes. The aim of this section is to consider aesthetic compromises and dilemmas and in doing so prevent less than optimal outcomes.
Outcome
On reading this section practitioners will be able to prevent aesthetic compromises and deal effectively with common aesthetic dilemmas.
Introduction
One thing certain in restorative dentistry is that all interventions and treatments, however well done, are ultimately likely to fail. Long-term failure is to be expected, and practitioners should be able to give an indication of the longevity of restorations. Arguably, without this information the consent process is not informed. Central to our understanding of aesthetic failures is that treatment can be well executed technically, yet the patient can deem it a failure for aesthetic reasons alone. It is important, therefore, to consider failures, and more importantly to judge how to foresee and prevent them. Various pitfalls and dilemmas with the aesthetics of anterior restorations will be considered.
Informed Consent
Essential to the consent process is a discussion of alternative procedures and a comparison of the risks, costs and benefits of the various options. Bear in mind that aesthetic dentistry is something that patients generally request rather than something they need. This is in contrast to dental treatment needed to secure oral health. Consequently, doing nothing is also a treatment option that must be both considered and discussed. It is helpful to outline alternative treatments for the management of unsightly anterior teeth in terms of increasing levels of intervention, outlining the risks, costs and benefits (Fig 7-1). If bleaching is a possible treatment option then central to the consent for bleaching procedures at the present time is informing the patient of the current legal status of bleaching. Without this information the consent is not informed.
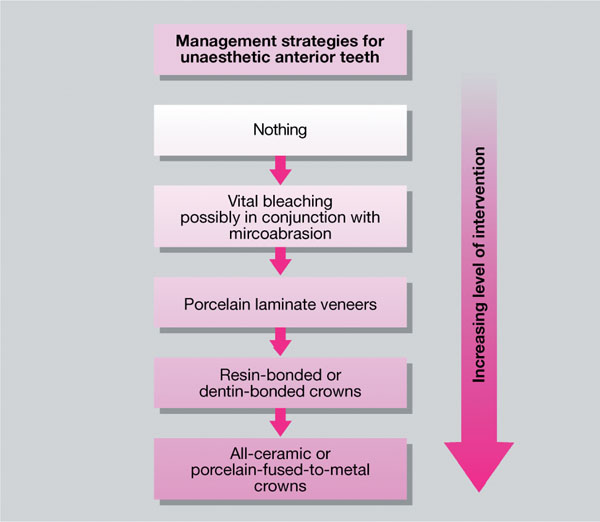
Fig 7-1 Management strategies for unaesthetic anterior teeth.
With aesthetic procedures it is important that what the patient requests and what treatment you can deliver are one and the same. Problems arise when this is not the case. Patients may attend seeking unrealistic treatments. Following a discussion as to what is possible, a course of action should be agreed and informed consent obtained. A written treatment plan should also be provided to the patient at this stage. Crucial to this process is an acceptance and understanding by the patient of what you have both agreed, – that is to say, what the treatment outcomes will be. If there is any doubt about this it might be prudent to decline to treat such patients.
The Single Tooth
Practitioners are not infrequently faced with the problem of a patient with a single discoloured or damaged tooth requesting treatment to improve their dental appearance. This is a difficult clinical scenario to manage effectively, especially if the tooth is intact.
Treatment options for a single discoloured tooth include:
-
doing nothing
-
bleaching
-
microabrasion, if appropriate, with or without bleaching
-
crowning or veneering the tooth.
Doing Nothing
Doing nothing is seldom an option when the patient has specifically requested treatment. However, it is important not to agree to provide treatment that is out of your range of skills and experience and you consider will have little, if any, chance of success or will be detrimental to the patient.
Bleaching
If the tooth is non-vital, management is relatively straightforward using a non-vital bleaching technique. If the tooth is vital and structurally sound, then a vital bleaching technique may be indicated. A modified bleaching technique is used in that carbamide peroxide is placed in the splint which may or may not have a reservoir, with the splint sectioned or cut away from the adjacent teeth. The cut-away limits the extent to which bleaching gel changes the colour of the adjacent teeth. This will usually work, but it is difficult to limit the whitening to the affected tooth. It is probably better to whiten the discoloured tooth and then whiten the entire arch, if appropriate, to compensate for collateral bleaching of adjacent teeth. If bleaching of the entire arch is not appropriate, a more controlled way of treating a single discoloured tooth is to use an in-surgery technique, accepting the limitations of this technique.
Microabrasion With and Without Bleaching
Microabrasion can be a useful technique for localised superficial discolorations. Localised discolorations affecting a single tooth that could be amenable to microabrasion are rare. The technique can be supplemented with in-surgery or night-guard vital bleaching as appropriate.
Crowning or Veneering the Tooth
Crowning possibly best treats the single discoloured tooth, including extensive restorations. Discoloured sound teeth that have failed to respond to bleaching or have an atypical shape may best be managed with a porcelain laminate veneer (Fig 7-2). The difficulty with single-unit aesthetic restorations is that it is almost impossible to match them successfully to adjacent sound teeth. Consequently it is preferable to treat pairs of anterior teeth with indirect restorations. This might mean an adjacent sound tooth being prepared, which flies in the face of a minimally interventive approach. To mitigate the effects of this a combination of a crown and veneer may be used (Fig 7-3). It is important in this situation that the patient understands why two teeth rather than one tooth need to be prepared.

Fig 7-2 Discoloured tooth that has failed to whiten with non-vital bleaching. This tooth will need either a veneer or, more correctly due its discoloration, a crown with a coping of either metal or ceramic.

Fig 7-3 (a) Patient with a single veneer on 21; the patient is unhappy with the appearance. (b) Replacement veneer for the patient illustrating how difficult it is to match one veneer.
Porcelain Laminate Veneers
Porcelain laminate veneers may be found to perform well in clinical service over a number of years if case selection, tooth preparation and placement techniques are optimal. Inevitably, all restorations, whatever their type, can deteriorate in clinical service. Central to remedying problems is an understanding of why the failure has occurred. Simply replacing the restoration will almost certainly result in a repeat failure, which will damage your confidence in the technique and your patient’s confidence in you. The various types of failure that can occur with porcelain laminate veneers are considered here, and the remedial action necessary either to repair the restoration or to ensure success with a replacement restoration is discussed. It is important to note that many of the failures that occur with porcelain laminate veneers may also occur with resin- or dentine-bonded crowns. The treatment required to remedy the fault is similar in most cases.
General Failure During Clinical Service
There is an increased incidence of failure of porcelain laminate veneers in teeth with (large) existing restorations. This occurs particularly when any existing restorations, notably proximal resin composite restorations, are not completely covered by the veneer. Extensive restorations require a hybrid-type preparation or, preferably, a complete coverage technique.
Loss of resin-luting cement can lead to catches, marginal staining, interfacial leakage and possibly caries that can be difficult to diagnose in its early stages. Equally, poor preparation technique can lead to problems with the emergence profile of the restoration. This can facilitate plaque accumulation, leading to a recalcitrant marginal gingivitis, which is difficult to resolve – not to mention poor anterior aesthetics.
Complete Loss
Complete loss of a porcelain laminate veneer may occur as a result of the following reasons:
-
Error in the use of the silane coupling agent; typically applying insufficient silane coupling agent – failure is likely to occur soon after cementation.
-
Improper wetting of the laminate by the resin-luting composite, possibly subsequent to contamination of the fitting surface during, for example, placement of />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


