6
Local anaesthesia in the lower jaw
6.1 Introduction
The buccal cortical bone at the premolars and molars of the lower jaw impedes the diffusion of anaesthetic fluid to the apices of these teeth, located centrally in the jaw bone. Adults require mandibular block anaesthesia for an effective anaesthesia. In the area of the lower canines and incisors the cortical bone is thinner and the roots lie on the buccal side of the jaw. Here, infiltration anaesthesia is effective.
The mental nerve leaves the jaw through the mental foramen and innervates the buccal mucosa and gingiva, the lower lip and the skin of the chin. Therefore, anaesthetising the mental nerve will not anaesthetise the teeth in adults. However, in children the molars are anaesthetised, because the apex of these teeth is reached through diffusion through the thinner cortical bone.
The lingual side of the mandible is innervated by the lingual nerve. This nerve can be anaesthetised both by block anaesthesia as well as by infiltration anaesthesia. The dentist must avoid pricking the floor of the mouth too often as this increases the risk of a haematoma in combination with transport of bacteria via the injection needle. This may cause a phlegmonous infection of the mouth floor, a life-threatening complication.
Block anaesthesia of the buccal nerve is possible. This nerve runs from high lingual and crosses the front side of the mandibular ramus above the occlusion plane. Then the buccal nerve continues caudo-ventrally to innervate the buccal mucosa and gingiva in the area of the (erupted) M3inf to P2inf. Because the height at which the buccal nerve crosses the mandibula varies, infiltration anaesthesia applied buccal to the respective teeth is also an excellent technique to anaesthetise the gingiva and mucosa (Figures 6.1 and 6.2).
Figure 6.1 The path of the mandibular nerve with its main branches.
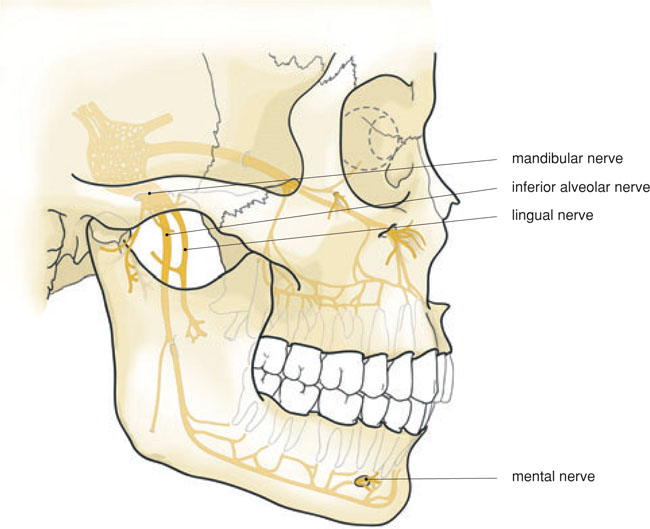
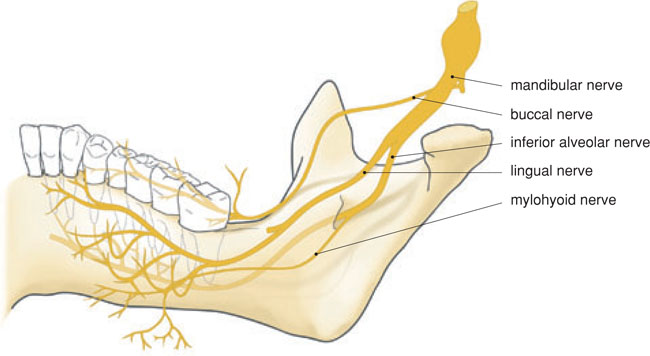
Figure 6.2 Medial aspect of the path of the mandibular nerve and its branches: the buccal nerve, lingual nerve and inferior alveolar nerve.
6.2 Incisors and canines
6.2.1 Anatomical aspects
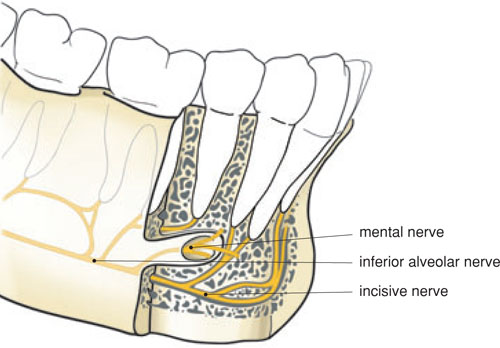
Once the alveolar nerve has separated from the trigeminal nerve, the nerve runs laterally and enters the mandibular foramen. The inferior alveolar nerve divides into a branch, the mental nerve, at the mental foramen and then continues as the incisive nerve. The incisive nerve no longer runs in a bony canal and divides into little branches leading to the roots of the lower canines and incisors (Figure 6.3). In the mandibular symphysis area, sensory anastomoses from the contralateral side are present, both lingually and buccally. This must be taken into account, particularly with extensive surgical treatment in the lower frontal area.
Figure 6.3 The path of the mental and incisive nerves.
The roots of the lower incisors and canines are found against the buccal cortical bone. The mental muscle is attached to the jaw at the height of the I2inf so that infiltration anaesthesia in this area can be painful and less effective.
6.2.2 Indication
Buccal infiltration anaesthesia will be sufficient for cavity preparations and endodontic treatment in the lower frontal area, unless a cofferdam and/or matrix band and wedges are used. In that case, it is necessary to apply additional anaesthesia lingually, or perhaps in the interdental papilla on the lingual side.
Infiltration anaesthesia is also used for surgical treatment in the lower frontal area, in which case the needle is inserted more caudally to the apex. The dentist must take the sensory anastamoses into account by also anaesthetising the contralateral nerve branches. The point of attachment of the mimic muscles, such as the orbicularis oris muscle and the mental muscle, also requires special attention during anaesthesia. Injecting into these muscles causes bleeding, is painful and does not lead to a good anaesthesia.
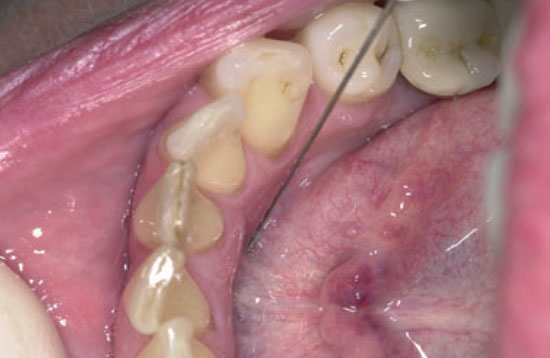
Figure 6.4 A and B Drawing (A) and photo (B) of infiltration anaesthesia of the I2 inferior right. The buccal gingiva is also anaesthetised. In order to anaesthetise the lingual gingiva, it is necessary to inject into the floor of the mouth.
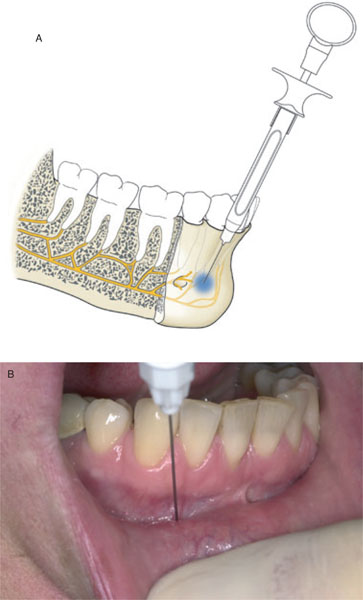
Figure 6.4 C Lingual anaesthesia with a bent needle with the dentist in an 8 to 9 o’clock position.

Figure 6.4 D Lingual anaesthesia with a non-bent needle with the dentist in an 11 to 1 o’clock position.
6.2.3 Technique
For infiltration anaesthesia in the lower frontal area, the non-injecting hand pulls the lip forwards and pinches the lip softly at the moment the needle penetrates the mucosa. The needle is inserted right under the apex of the tooth that is to be anaesthetised, up to the bone. Preferably, the needle is inserted vertically and not pushed into the periosteum. The dentist sits or stands behind the patient in an 11–1 o’clock position. The same position is assumed for infiltration anaesthesia of the lingual mucosa and gingiva. When anaesthetising from an 8–9 o’clock position, it is better to bend the needle 45–90 degrees for a lingual injection (Figure 6.4), but a disadvantage of this is that the needle cannot be returned to its protective cap. With lingual anaesthesia it is important to prevent a haematoma occurring.
Bilateral mandibular block anaesthesia, with additional local infiltration anaesthesia, is recommended for surgical treatment of the lower front, such as extensive pre-implantological treatments (e.g. a chin bone transplant) and implantological treatments (two or four dental implants). This reduces the required number of injections to a minimum, as well as the chance of haematomas and infections. Furthermore, a maximum of 4–6 ml of anaesthetic fluid will be sufficient.
In this situation it is recommended that the dentist administers the double-sided mandibular block first and then waits until the patient spontaneously indicates that the lower lip and border of the tongue have started to tingle. The dentist can then give a buccal infiltration anaesthesia.
6.3 Premolars
6.3.1 Anatomical aspects
Innervation of the premolars in the lower jaw takes place in the bone through the inferior alveolar nerve, buccal through the buccal nerve (at the P1inf also through the mental nerve) and lingually through the lingual nerve. Because of the thickness and impermeability of the buccal cortical bone, infiltration anaesthesia is not really possible for the treatment of the (pulpa of) premolars in adult patients.
Use of block anaesthesia of the mandibular nerve, i.e. of the inferior alveolar and lingual nerves, is therefore a more obvious choice, if necessary supplemented with local infiltration anaesthesia of the branches of the buccal nerve (Figure 6.5). The mental nerve is found lower than the apices, exactly between the two premolars. Block anaesthesia of the mental nerve branches must be given superficially to avoid damage to the mental nerve, with subsequent long-term anaesthesia of the lower lip half.
If a combination of bloc/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


