Facial Sculpture
Claude R. Rufenacht
Striated muscle: Physical and physiologic characteristics
The muscle fiber represents the basic unit of voluntary striated muscles.1 Surrounded by an isolating connective tissue sheath, each muscle fiber may contract while the others remain inactivated. Bound together in bundles, supplied by nerves, lymph, and blood vessels, striated muscle fibers do not increase in number after birth; they only increase in diameter.
When a muscle fiber is stimulated, it contracts to its full extent; then, according to the strength of the demand, other fibers may contract. The muscle fiber is either fully contracted or fully relaxed.
In comparison with the muscle fiber, a muscle is always in a state of slight contraction. This apparent contradiction can be explained by the connection of the fibers with each other and the fact that the muscle fibers do not run the full length of the muscle. In a normal resting muscle certain fibers are fully contracted bringing a slight degree of tension to the entire muscle until they tire and are replaced by the contraction of other fibers. This process of maintaining a slight tension is called muscle tone.2
Muscle tone can also be defined as the passive resistance of muscles to stretch. In an increased passive resistance to stretch, muscles are said to be hypertonic, whereas in reference to a diminished passive resistance, they become hypotonic.
Reflex action
Muscle activity is the result of a reflex action in which impulses are transmitted to the brain by means of proprioceptive nerves where they are converted into stimuli that pass by way of motor fibers into the muscle where the response is an involuntary or automatic contraction.3 For example, the tension exerted on the muscles of depression in the phenomenon of gravity stimulates the elevators and brings them into a state of slight contraction. In a similar fashion, the constant contraction of the elevators stimulates the depressors. This reflex action is called stretch reflex or myotatic reflex.2,4 This explains the maintenance of the mandible in the rest position and the upright function of the head when no activity is present.
Muscle tonus is that part of muscle tone resulting from the myotatic reflex.2 However, in a general sense, passive properties, such as the elasticity of the muscle and the surrounding tissues, and the myotatic reflexes, participate in the muscle tonus.
Muscle tonus and myotatic reflexes can be influenced and altered by inhibition or facilitation of the gamma or alpha motoneurons. As a result, a variety of factors, including psychologic, physical, emotional, and physiologic states, will affect muscle tonus.5
The muscular contractions that are at the base of muscular activity are of the same nature and differ from myotatic reflex only by the number of fibers that are activated.
Muscular activity as the result of myotatic reflex remains totally unconscious. When part of the impulses that are conveyed to the brain reach a level of consciousness, they are relayed to the voluntary motor area and are converted into voluntary or intentional motor stimuli that generate a voluntary contraction.
The physiologic principles of muscular6 contraction may be summarized as follows:
1. When a single muscle fiber is activated, it contracts completely before a second fiber can contract.
2. Muscles are in a constant state of slight contraction (myotatic reflex).
3. The amount of strength produced by a muscle depends upon the number of fibers activated.
4. Muscles work in pairs. When a muscle contracts, the antagonist relaxes.
Movements occur through paired muscular activity and the individual muscle functions by being (1) a prime mover or initiator of the movement; (2) an antagonist, which relaxes when the mover contracts; (3) a fixator, in which a muscle establishes a stable basis for future complementary movement; and (4) a synergist, which may help the prime mover in its action.
The physiologic principles of muscular contraction and the movements exhibited during muscle function imply two types of muscle activity, dynamic and static7,8 (Fig 6-1).
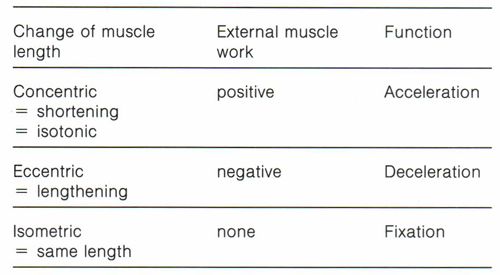
Fig 6-1 Diagram of muscular activity. From Christensen.7
Dynamic muscle activities are divided into concentric contraction with shortening of the muscle fiber and production of positive work, and eccentric contraction with lengthening of the muscle fiber and production of negative work.9 During positive work muscle tension overcomes external forces, whereas in negative work external forces overcome muscle tension.
Static muscle activity produces isometric contraction and takes place when variable levels of tension are exerted at a constant length of the fiber, such as maintaining weights immobile during the range of lifting movement.
Muscle motion mainly exhibits elements of dynamic and static activity. Pure static or dynamic contraction is difficult to find in nature.
Facial muscles, highly integrated with one another, are characterized by a large variability in size and shape from one individual to another.
The absence of fascia and the integration of the fiber bundles explain the variety of combinations and the modulation of activity that takes place during facial expressions and express the characteristics of an individual, making him or her a distinct entity. The loss of these characteristics that may produce an important psychologic impact may become inevitable when facial movements requiring dental participation are affected by intraoral pathologies.
Subtle and highly individual facial expressions require the selected contraction of certain facial muscles, easily visualized by means of their delicate fibers or tendons attached to the skin and mucosa of the lip. They can show a variety of psychologic states10,11 so that their meaning is clearly recognized and understood.12
The implication of movements of the lips, cheeks, and tongue during the movements of mastication and deglutition can be easily visualized, and a similar implication of coordinate movements of the mandible in the production of speech and facial expressions has been demonstrated. This suggests that unless strictly classified, none of the muscles involved in human oral and facial functions are totally independent13 so that prosthodontists must recognize the importance of function in terms of restoration of movements of mastication, deglutition, speech, facial movements, and movements of expression.
The meticulous and progressive restoration of the dentogingival unit, tooth arrangement, vertical dimension, occlusion, and function is naturally integrated in daily practice.
If we accept the postulate that dental esthetics implies the restoration of the dentofacial environment, facial muscles that are part of its constitutive elements should receive attention proportionate to their esthetic and functional importance. Muscle retraining techniques that are aimed at putting back in action muscles or a group of muscles, which for any reason have lost their full range of activity and undergone atrophic changes, totally fulfill these requirements. Therefore, systematic recourse to these techniques, as a condition for a complete improvement of facial appearance, should be considered following any type of dental rehabilitation. However, one should keep in mind that improvement will only be obtained if the programmed aging process that throughout life erodes the integrity of the orofacial unit has not gone too far. This sequence of therapeutic techniques has to be respected before the patient can be referred to the specialist as a potential candidate for rhytidectomy. Conversely, some consideration of the facial implication of oral pathologies can be expected from plastic surgeons.
In integrating the muscle retraining techniques in the framework of the daily home care program, we ascribe to these techniques their true significance, which is the maintenance of a healthy dentofacial environment and a youthful appearance.
According to Martone and Edwards,14 the head and neck are divided into two distinct regions: fixed in the upper part of the face and movable in its lower part. Whereas the muscles of the upper part of the face exhibit limited facial movements, the movable lower bone region, depicted as an inverted pyramid extending from the sternum to the ears, houses the muscles that generate, in whole or in part, the functions of mastication, deglutition, speech, and a variety of facial expressions that involve oral participation. Knowledge of the muscles of the perioral structures that contribute to the movements of the lips and understanding of their range of action are prerequisites for the appropriate use of these techniques.
From a diagrammatic illustration, one can observe a bilateral convergence of a number of muscles toward the corner of the mouth where they form an interlacing knot called modiolus, approximately situated at the level of the first or second mandibular premolar (Fig 6-2). This thick, 3- to 4-mm-deep mass, which is extremely mobile and can be instantly and voluntarily moved or fixed by the synergic action of several of the facial muscles that interlace at this point of convergence,15 has been recognized and described by prosthodontists.16
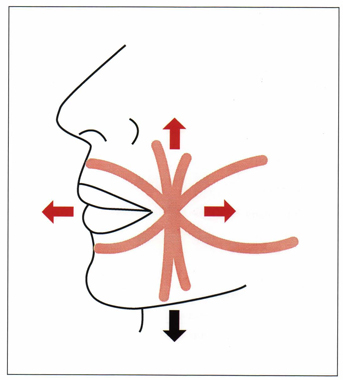
Fig 6-2 The modiolus, muscular knot in which mainly buccinator and orbicularis oris, caninus and triangularis oris, and zygomaticus interlace.
These muscles (Fig 6-3) in association with other facial muscles, are involved in the production of six types of movements that can be visualized in this area, comprising the participation of the muscles in Table 6-1.
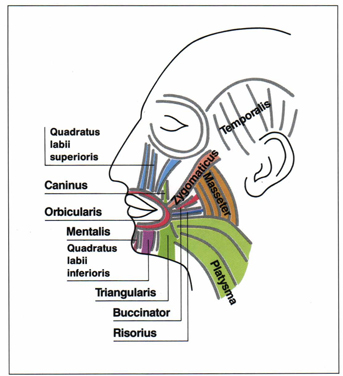
Fig 6-3 The muscles of facial expression.
This variety of facial movements always involves dental participation through the active contribution of the modiolus and the orbicularis oris.
The maintenance of a firm face that is the privilege of youth becomes the symbol of physical health, vigor, and efficiency associated with that period of life, whereas older individuals usually exhibit sagging and wrinkles. The sagging of the face that cannot be totally explained through the phenomenon of gravity indicates that facial muscles are not used to their full capacity. Muscle conditioning, training, and strengthening through dai/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


