Chapter 5
Porcelain Laminate Techniques
Aim
Porcelain laminate veneer techniques have not been popular with certain practitioners, possibly because they have given poor results in comparison with those obtained by more traditional full-coverage techniques. The aim of this chapter is to reconsider porcelain laminate veneer restorations and consider how they can be used to good effect in modern-day aesthetic dentistry. The advantages of porcelain laminate veneers when compared to full-coverage techniques are also considered.
Outcome
On reading this chapter practitioners will be familiar with the indications, contraindications, advantages and disadvantages of porcelain laminate veneers along with the clinical techniques necessary to achieve optimal results with restorations of this type.
Introduction
The acid-etch technique was first described by Michael Buonocore in 1955. Rochette realised the potential of this for the micromechanical attachment of resin-based materials in 1973 and used the technique for the splinting of periodontally involved lower anterior teeth. Some ten years later porcelain-etching and the use of silane-coupling agents were concurrently described. The combined effects of these innovations have been that predictable outcomes for resin-bonded restorations are now possible for practitioners. These restorations can be bonded into place, which opens up opportunities for minimally interventive restorations (for example, porcelain laminate veneers).
Historical Perspective
Dr Charles Pincus first described Hollywood veneers in 1948. He used the technique to improve the appearance of teeth for actors and actresses, notably Shirley Temple. The veneers were held in place with denture adhesive and were removed after filming. Hollowed-out acrylic denture teeth, which failed, given a poor bond between the acrylic and resin composite, have been tried in the past. Similarly, preformed acrylic veneers marketed by Caulk in the 1980s tended to fail as a consequence of a poor bond between the acrylic and luting resin composite. Microfine resin composites have also been used, but these failed due to poor wear resistance, polymerisation shrinkage and inferior aesthetics with stain build-up. Porcelain veneers were first described in 1983 and introduced into the UK in 1984. Although porcelain is the material of choice, it should be noted that direct and indirect resin composite veneering techniques still have a place in the treatment of adolescent patients as intermediate restorations.
Indications
Porcelain laminate veneers are thought to be indicated in the following situations:
-
Treatment of unsightly surface defects in essentially sound anterior teeth.
-
Modifications to anterior tooth colour, shape, length and alignment.
-
Restoration of fractured and endodontically treated anterior teeth.
-
Treatment of anterior teeth with hypoplastic enamel.
-
Masking discoloration caused by trauma, endodontic treatment, fluorosis and tetracycline staining (Fig 5-1).
-
Repair of damage to anterior teeth, such as fractured incisal edges.
-
Masking anatomical anomalies, including peg-shaped laterals (Fig 5-2).
-
Treatment of amelogenesis imperfecta but not dentinogenesis imperfecta, as the enamel is prone to fracture off in the latter condition, leading to early failure of the restorations.
-
Closure of a median diastema, although this can be achieved quite easily with direct application of resin composite in carefully selected cases.

Fig 5-1 (a) Tetracycline staining. (b) Same patient with porcelain laminate veneers.
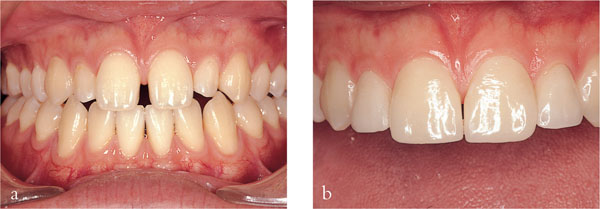
Fig 5-2 (a) Patient with a diastema and abnormally shaped lateral incisors. (b) Same patient with veneers in place.
Contraindications
In contrast, porcelain laminate veneers are contraindicated in the following clinical situations:
-
Poor oral hygiene.
-
Where the restoration would have to have deeply placed subgingival margins.
-
Atypical occlusal loading (for example, bruxism).
-
Lack of adequate amounts of tooth tissue for bonding or poor-quality enamel, albeit in adequate amounts.
-
Presence of large existing restorations, which favour a full coverage technique, as failure rates for porcelain laminate veneers placed on teeth with existing restorations are reported to be high.
Advantages
It is generally accepted that porcelain laminate veneers have the following advantages:
-
Minimally interventive, especially when compared with full coverage restorations.
-
Local analgesia is not normally required for tooth preparation or placement of the veneers.
-
The aesthetic outcome can be exceptional.
-
Typically no provisional restoration(s) are required.
Disadvantages
-
Not a reversible technique, although previously thought to be, which is partly responsible for the confusion regarding the nature of preparation required.
-
Relatively limited application, given that the tooth or teeth should be essentially intact.
-
Technique sensitivity, in particular demanding preparation criteria and moisture control at placement.
-
Long-term data are somewhat limited but encouraging – porcelain laminate veneers can reasonably be expected to last at least three years but clinical experience suggests that clinical service is typically in excess of five to 10 years.
-
Poss/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


