DEFINITION
SITES OF DENTAL CARIES
• Pathogenic Properties of Cariogenic Bacteria and Pathogenesis of Dental Caries
• Hypothesis Concerning Relation between Plaque and Caries
THEORIES OF DENTAL CARIES
• Acidogenic Theory
• Proteolytic Theory
• Proteolysis-chelation Theory
• “Caries Balance Concept” (Proposed by Featherstone)
LOCAL FACTORS AFFECTING THE INCIDENCE OF CARIES
• The Host
• Environment of the Tooth: Saliva and Diet
• The Bacteria
• Time Period
CLASSIFICATION OF DENTAL CARIES
• According to their Anatomical Site
• According to Whether it is a New Lesion or Recurrent Carious Lesion
• According to the Activity of Carious Lesion
• According to Speed of Caries Progression
• Based on Treatment and Restoration Design
• Based on Pathway of Caries Spread
• Based on Number of Tooth Surfaces Involved
• Classification According to the Severity
• Graham Mount’s Classification
HISTOPATHOLOGY OF DENTAL CARIES
• Caries of Enamel
• Caries of Dentin
DIAGNOSIS OF DENTAL CARIES
• Visual-Tactile Method of Diagnosis
• Radiographic Method of Diagnosis
CARIES RISK ASSESSMENT
PREVENTION OF DENTAL CARIES
• Methods to Reduce Demineralizing Factors
• Methods to Improve Oral Hygiene
• Chemical Measures
• Methods to Increase Protective Factors
CURRENT METHODS OF CARIES PREVENTION
• Genetic Modalities in Caries Prevention
• Caries Vaccine
MANAGEMENT OF DENTAL CARIES
DEFINITION
Dental caries is defined as a microbiological disease of the hard structure of teeth, which results in localized demineralization of the inorganic portion and destruction of the organic substances of the tooth.
Cariology is a science which deals with the study of etiology, histopathology, epidemiology, diagnosis, prevention and treatment of dental caries.
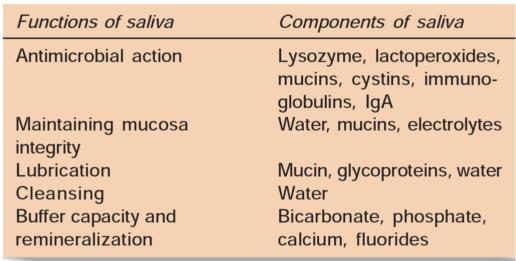
SITES OF DENTAL CARIES (FIGS 4.1A TO F)
As we know that plaque is the essential forerunner of caries and therefore the sites on the tooth surface which encourage plaque retention and stagnation are particularly prone to progression of lesions. These sites are:
• Pits and fissures on occlusal surfaces of molars and premolars.
0 Buccal pits of molars.






Figs 4.1A to F: Most common sites of caries development
• Palatal pits of maxillary incisors.
• Enamel of the cervical margin of the tooth just coronal to the gingival margin.
• Proximal enamel smooth surfaces apical to the contact point.
• In teeth with gingival recession occurring because of periodontal disease.
• The margins of restorations predominantly which are deficient or overhanging.
• Tooth surfaces adjacent to dentures and bridges.
Pathogenic Properties of Cariogenic Bacteria and Pathogenesis of Dental Caries
Cariogenic bacterias have some characteristics which make them special:
• Acidogenic nature: This means bacterias should be able to transport sugars and convert them to acid.
• Aciduric nature: Bacterias should be able to thrive at low pH.
– Bacterias should be able to produce extracellular and intracellular polysaccharides which contribute to the plaque matrix. These intracellular polysaccharides can be used for energy production and converted to acid when sugars are not available (Fig. 4.2).
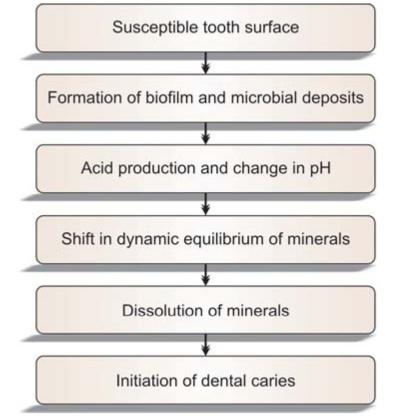
Fig. 4.2: Pathogenesis of dental caries
Hypothesis Concerning Relation between Plaque and Caries
• The specific plaque hypothesis says that only a few organisms out of the diverse collection in the plaque flora are actively involved in the disease. Preventive measures against these bacteria can control occurrence of the disease.
• The non-specific plaque hypothesis believes that the carious process is caused by the overall activity of the total plaque microflora. Accordingly all plaque should be removed by mechanical plaque control.
• The ecological plaque hypothesis says that the organisms associated with disease may be present at sound sites. Demineralization results if there is shift in the balance of these resident microflora by a change in the local environment. Frequent sugar intake encourages the growth of acidogenic and aciduric species, thus predisposing to caries. According to this hypothesis, both mechanical cleaning and restriction of sugar intake are important in controlling caries progression.
THEORIES OF DENTAL CARIES
As we know, dental caries is a multifactorial disease of tooth which has been explained by many theories. Though there is no universally accepted theory of the etiology of dental caries, but following three theories are considered in etiology of dental caries:
1. Acidogenic theory
2. Proteolytic theory
3. Proteolysis-chelation theory.
Acidogenic Theory
• WD Miller was the first known investigator of dental caries. He published his results in 1882.
• This theory is most accepted.
• Miller said “Dental decay is a chemico-parasitic process consisting of two stages, the decalcification of enamel, which results in its total destruction, as a preliminary stage; followed by dissolution of the softened residue of the enamel and dentin.
• In the first stage there is destruction which is done by the acid attack where as the dissolution of the residue (2nd stage) is carried out by the proteolytic action of the bacterias.
• This whole process is supported by the presence of carbohydrates, microorganisms and dental plaque.
• All the preventive steps have been based on this theory.
The Role of the Dental Plaque
Dental plaque also known as microbial plaque is important for beginning of caries because it provides the environment for bacteria to form acid, which causes demineralization of hard tissue of teeth.
Proteolytic Theory
• Heider, Bodecker (1878) and Abbott (1879) thrown considerable light to this theory.
• According to this theory, organic portion of the tooth plays an important role in the development of dental caries.
• It has been recognized that enamel contains 0.56% of organic matter out of which 0.18% is keratin and 0.17% is a soluble protein.
• Enamel structure which are made of the organic material such as enamel lamelle and enamel rods prove to be the pathways for the advancing microorganisms.
• Microorganisms invade the enamel lamelle and the acid produced by the bacterias causes damage to the organic pathways.
Proteolysis-chelation Theory
This theory was put forward by Schatz and his coworkers.
Chelation
• It is a process in which there is complexing of the metal ions to form complex substance through coordinate covalent bond which results in poorly dissociated/or weakly ionized compound. Example of chelation reaction is hemoglobin in which 4 pyrrole nuclei are linked to iron by a similar bond.
• Chelation is independent of the pH of the medium.
• Bacterial attack on the surface of the enamel is initiated by keratinolytic microorganisms. This causes the breakdown of the protein chiefly keratin. This results in the formation of soluble chelates which decalcify enamel even at neutral pH.
• Enamel contains mucopolysaccharides, lipids and citrate which are susceptible to bacterial attack and act as chelators.
Reduced incidence of caries because of fluoridation has been explained by this theory. According to this, due to formation of fluoroapatite, strength of linkage between organic and inorganic phases of enamel is increased which helps in reducing their destruction.
“Caries Balance Concept” (Proposed by Featherstone) (Fig. 4.3)
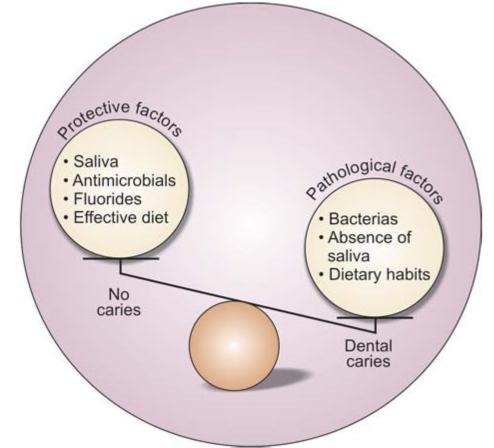
Fig. 4.3: Caries balance concept. If pathological factors overweight then caries progress
According to the caries balance theory, caries does not result from a single factor; rather, it is the outcome of the complex interaction of pathologic and protective factors. Pathological factors involved in a carious lesion are bacteria, poor dietary habits, and xerostomia. Protective factors include saliva, antimicrobial agents (chlorhexidine, xylitol), fluoride, pit and fissure sealants and an effective diet.
A balance between pathologic and protective factors dynamically changes throughout the day, even in healthy individuals. Any change in balance of these factors can result in carious lesion. So these risk factors must be evaluated from time-to-time because the effect of each factor can change over time. For example, if a person is healthy today and develops xerostomia, he can develop severe decay months later.
LOCAL FACTORS AFFECTING THE INCIDENCE OF CARIES (FIG. 4.4)
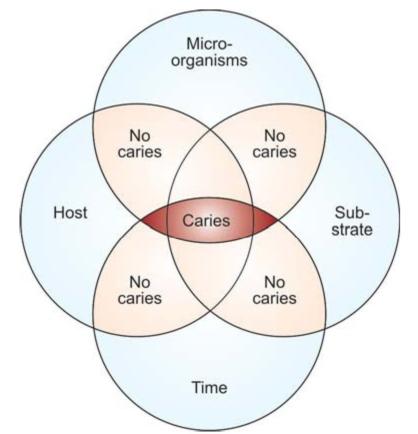
Fig. 4.4: Factors affecting incidence of dental caries
Dental caries is an ecological disease in which the diet, the host and the microbial flora interact in a way which increases demineralization of the tooth structure with resultant caries formation.
Some races have higher incidence of dental caries, e.g. white American and English people. Some races (e.g. Indians and black Americans) due to hereditary patterns have lower incidence of dental caries. There are some local factors which can easily alter the manifestation of caries activity based on heredity pattern.
The difference in occurrence of dental caries in different individuals of same age, sex, race and geographic area, diet, and similar living conditions is because of various factors that manipulate the etiology of caries.
1. Tooth (Host)
a. Variation in morphology
b. Composition
c. Position
2. Substrate (Environmental factors)
a. Saliva
i. Composition
ii. Quantity
iii. PH
iv. Viscosity
v. Antibacterial factors
b. Diet
i. Physical factors
ii. Local factors
• Carbohydrate content-presence of refined cariogenic carbohydrate particles on the tooth surface
• Vitamin content
• Fluoride content
• Fat content
3. Microorganisms-most commonly seen microorganisms associated with caries are Streptococcus mutans and Lactobacillus.
4. Time period
The Host
• Lack of enamel maturation or the presence of developmental defects in enamel may result in increase the caries risk. These defects increase plaque retention, increase bacterial colonization, and in some cases, the loss of enamel make it more susceptible to tooth demineralization.
• The physical characteristics of teeth like deep and narrow occlusal fissures, deep buccal or lingual pits and enamel hypoplasia, etc. affect the initiation of dental caries.
• Fluoride content is lesser in carious enamel and dentin as compared to a sound tooth. In carious enamel and dentin it is 139 ppm and 223 ppm, whereas in sound enamel and dentin it is 410 ppm and 873 ppm, respectively.
• If a tooth is out of position, rotated or in any abnormal position, it becomes difficult to clean, and hence retains more food and debris.
Environment of the Tooth: Saliva and Diet
Saliva
• Saliva contains salivary proteins which get deposited onto the tooth surface which help the enamel against acid dissolution. This protective layer is referred to as the pellicle.
• Since saliva is rich in calcium, phosphate and fluoride, these materials help in remineralization of the enamel.
• Saliva acts as cleaner of teeth as it quickly washes away food debris from the mouth and to buffer the organic acids that are produced by the bacteria.
• Any salivary dysfunction, effect of medication or radiotherapy can result in decreased quantity and quality of saliva which further promotes caries.
• When salivary flow is reduced or absent, there occurs the increased food retention. Since salivary buffering capacity is lost, an acid environment is encouraged which further promotes the growth of aciduric bacteria. These aciduric bacterias savor the acid conditions and metabolize carbohydrates in the low-pH environment. This results in initiation of the caries.
Diet (Fig. 4.5)

Fig. 4.5: Physical nature of diet affects the incidence of dental caries
•Physical nature ofdiet: In the earlier times, the primitive man used to eat rough and raw unrefined foods which had self-cleansing capacity. But in present times, soft refined foods are eaten which stick stubbornly to the teeth and are not removed easily due to lack of roughage. This is the reason for higher incidence of dental caries nowadays than the past.
•Nature of carbohydrate content of the diet: To cause demineralization of dental enamel, it is essential for fermentable carbohydrates and plaque to be present on the tooth surface for a minimum length of time. These need to be retained in the mouth long enough to be metabolized by oral bacteria to produce acid.
•It is seen that acids produced by fermentable carbohydrates cause a rapid drop in plaque pH to a level which results in demineralization of the tooth structure. But since acids produced in plaque diffuse out of the plaque combined with buffering capacity of saliva exerting a neutralizing effect, this acidic nature of plaque remains for sometime only, and with in 30-60 minutes, plaque returns to its normal pH. However, repeated and frequent consumption of sugar will keep plaque pH depressed which results in demineralization of the teeth. Stephan has shown the relationship between change in plaque pH over a period of time following a glucose rinse in form of a graph. This graph is called a “Stephan curve” (Stephan and Miller, 1943) (Fig. 4.6). The drop in pH is the result of fermentation of carbohydrates by plaque bacteria. The gradual return of the pH occurs because of buffers present in plaque and saliva. This drop in pH can demineralize tooth structure depending on the absolute pH decrease, as well as the length of time that the pH is below the “critical pH” level. The critical pH value for demineralization usually ranges between 5.2 to 5.5. Caries occurs when the process of remineralization is slower than the process of demineralization and there is a net loss of mineral into the environment. It can be prevented by restricting the intake of dietary sugars, and removing plaque.
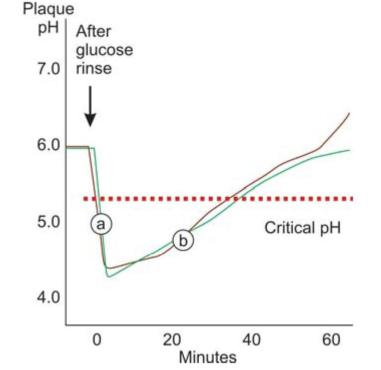
Fig. 4.6: Stephan curve graph showing plaque pH before and after glucose rinse. (a) pH decreases because of acids produced by bacteria, (b) pH increases, due to buffering of plaque and saliva
Tooth remineralization can take place if the pH of the environment adjacent to the tooth is high due to:
• Lesser number of cariogenic bacteria
• Availability of fluoride
• Lack of substrate for bacterial metabolism
• Elevated secretion rate of saliva
• Strong buffering capacity of saliva
• Presence of inorganic ions in saliva
• Quick washing of retained food.
• Frequency of carbohydrate intake: In a person with normal salivary function, after intake of fermentable carbohydrate foods or drinks, the acidic pH lasts 30-60 minutes. Greater time between acid attacks allows greater time for the repair process (remineralization) to occur.
• Vitamin content of the diet: As we know vitamin are essential components of daily diet. Deficiency of some vitamins increases the incidence of dental caries.
VitaminA:Deficiency or excess are not related to dental caries.
VitaminD:Vitamin D helps in normal development of teeth. Enamel hypoplasia can result due to vitamin D deficiency. It can result in early attack of caries. It has been seen that supplement of vitamin D in children helps in the formation of healthy teeth and thus helps in reduction in the dental caries.
VitaminK.Deficiency does not affect the dental caries incidence.
VitaminBItsdeficiency may exert a caries protective
complex:influence on the tooth. Several types of vitamin B are important growth factors for the oral acidogenic flora which serve as component of the co-enzymes involved in glycolysis. Vitamin B6 acts as an anticaries agent because it promotes the growth of noncariogenic organisms.
VitaminC:Directly vitamin C does not help in protection of tooth against dental caries, but it is required for the normal health of the gingiva.
The Bacteria
• Dental caries do not occur if the oral cavity is free of bacteria.
• Most commonly seen bacterias associated with caries are Streptococcus mutans, Lactobacillus spp., Veillonella spp. and Actinomyces spp.
• Streptococci mutans are considered main causative factors for caries because of their ability to adhere to tooth surfaces, produce abundant amounts of acid, and survive and continue metabolism at low pH conditions. Colonization with Streptococcus mutans at an early age is an important factor for early caries initiation.
Time Period
The time period during which all above three direct factors, i.e. tooth, microorganisms and substrate are acting jointly should be adequate to produce acidic pH which is critical for dissolution of enamel to produce a carious lesion. Time required for acid production from the fermentation of the carbohydrates by bacteria and for demineralization of tooth, is allowed by poor oral hygiene and not cleaning teeth immediately after eating.
CLASSIFICATION OF DENTAL CARIES
Carious lesions can be classified in different ways.
According to their Anatomical Site
• Pit and fissure caries (Fig. 4.7): Pit and fissure caries occur on occlusal surface of posterior teeth and buccal and lingual surfaces of molars and on lingual surface of maxillary incisors.
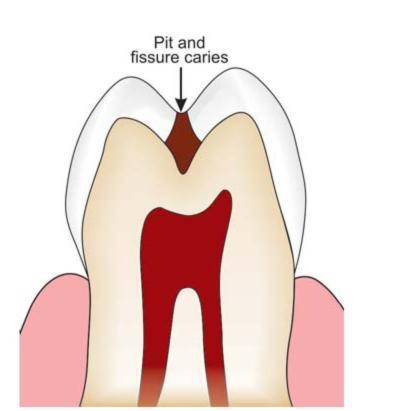
Fig. 4.7: Pit and fissure caries
• Smooth surface caries (Fig. 4.8): Smooth surface caries occurs on gingival third of buccal and lingual surfaces and on proximal surfaces.
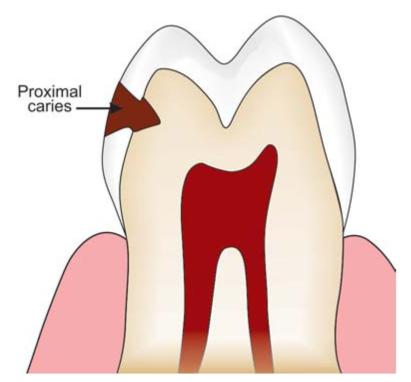
Fig. 4.8: Smooth surface caries
• Root caries (Fig. 4.9): When the lesion starts at the exposed root cementum and dentin, it is termed as root caries.
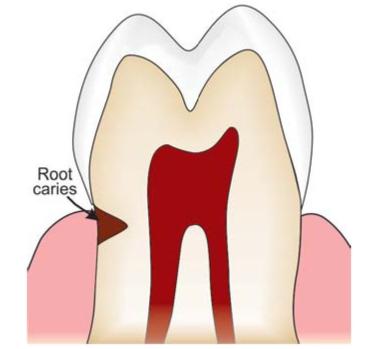
Fig. 4.9: Root caries
According to Whether it is a New Lesion or Recurrent Carious Lesion
• Primary caries denotes lesions on unrestored surfaces (Fig. 4.10).

Fig. 4.10: Primary caries
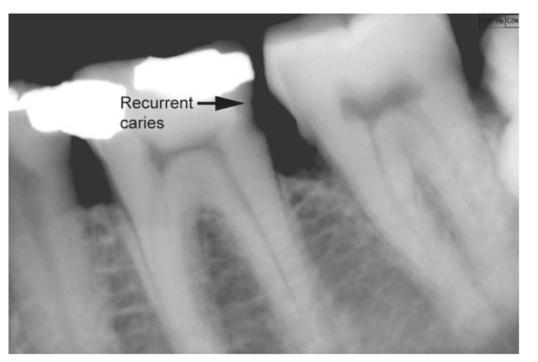
• Recurrent caries (Fig. 4.11): Lesions developing adjacent to fillings are referred to as either recurrent or secondary caries.
Fig. 4.11: Radiograph showing recurrent caries adjacent to proximal restoration
• Residual cariesis demineralized tissue left in place before a filling is placed (Fig. 4.12).
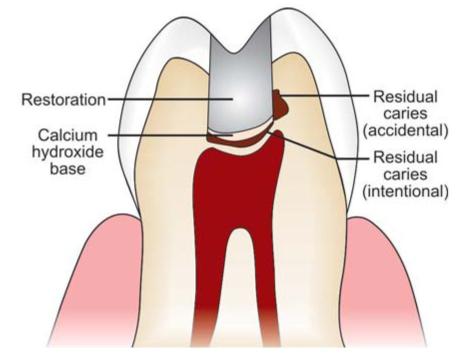
Fig. 4.12: Residual caries
According to the Activity of Carious Lesion
• Active carious lesion: A progressive lesion is described as an active carious lesion.
• Inactive/arrested carious lesion: A lesion that may have formed earlier and then stopped is referred to as an arrested or inactive carious lesion. Arrested carious lesion is characterized by a l/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


