41
Stability and retention
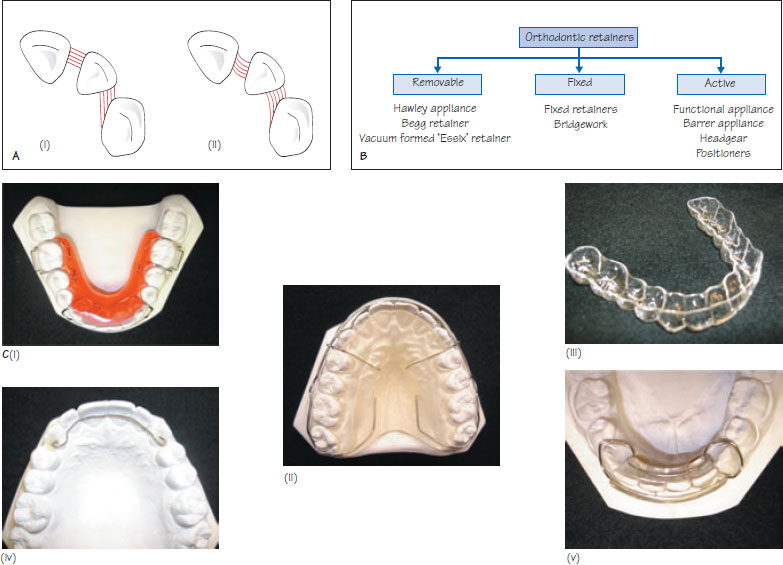
Figure 41.1 (A) (i) The transseptal fibres (shown in red) are an important cause of relapse of derotated teeth because of the long interval required for the fibres to reorganise following tooth movement, (ii) Derotation results in stretching of the fibres with generation of forces of elastic recoil. (B) A classification for orthodontic retainers. (C) Examples of orthodontic retainers: (i) Hawley retainer, (ii) Begg retainer, (iii) vacuum formed Essix-type retainer, (iv) fixed retainer and (v) Barrer spring retainer.
Orthodontic relapse is the term given when features of the original malocclusion return following the active phase of treatment. Retention is the phase of treatment following active tooth movement that is aimed at stabilising corrected intra-arch and inter-arch relationships. Retention should be planned during the treatment planning stage and discussed in detail as part of informed consent.
Orthodontic stability
Poor stability may occur for a number of reasons following treatment including:
- periodontal recovery;
- soft tissue imbalance;
- skeletal growth.
Orthodontic tooth movement results in disruption of the periodontal and gingival structures. Because these tissues are slow to remodel following orthodontic tooth movement, residual tension within the periodontal ligament and gingival fibres results in elastic recoil which moves teeth towards their pre-treatment position. To prevent relapse it is important to maintain the corrected positions until reorganisation is complete. Following appliance removal it takes approximately 3–4 months for the principal periodontal fibres, 4–6 months for the gingival fibres and 1 year for the transseptal fibres to reorganise if subjected to normal masticatory loading. Because of slow reorganisation of the transseptal fibres, derotated teeth are particularly prone to relapse (Figure 41.1A) and consideration should be given to long-term retention for severe rotations. Pericision may help to reduce the relapse of derotated teeth in the short term, however, the long-term benefits are questionable. This procedure involves surgically cutting the disrupted transseptal fibres by making a gingival crevicular incision under local anaesthesia following alignment.
If teeth are moved into an inherently unstable position during treatment, pressure from the soft tissues, such as the lips, cheeks and tongue, may result in relapse. This may occur if the lower incisors are excessively (>2 mm) advanced/proclined, if the dental arches are expanded out of soft tissue balance, and if the upper incisors are not controlled by the lower lip following incisor retraction (Class II cases). If such movements are undertaken intentionally, long-term retention should be planned at the treatment planning stage and discussed as part of informed consent.
The skeletal growth pattern existing before orthodontic treatment is lik/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


