Structural Esthetic Rules
Claude R. Rufenacht
Facial features
Although orthodontists have established a rule of sagittal norms, frontal norms do not really exist and any attempt to define frontal beauty based on biometric measurements would not be valid because of the limitations imposed by the variety of racial, ethnic, and individual types.
The combination of the numerical quantification of beauty postulated by Greek philosophers with beauty’s psychophysical quantification has been advocated as being a more pertinent approach to the evaluation of human esthetics.
In introducing the presumption of the individuality of human beauty, a strict definition of frontal facial norms loses meaning because beauty depends upon esthetic and morphopsychologic principles imposed by the equilibrium existing between facial zones and the harmonious integration of the receptors.
Disturbances affecting this equilibrium as a result of our genetic heritage and environmental compulsions can be corrected or attenuated by means of dentofacial orthopedic or reconstructive surgery.
The frequency of accidental aging events and the programmed progression of age affecting facial esthetic equilibrium will also call for therapy and require the multidisciplinary approach of diverse branches of medicine and paramedicine, keeping in mind that in this field of interest morphologic changes involve skin, facial adipose tissue, aponeurosis, muscles, teeth, and facial skeleton.
The presence of grooves perpendicular to the direction of the pull of the muscles is a constant of facial anatomic features. They are more or less marked depending upon the individual, and their permanence is basically linked to the nature of the tegumental relief and the degree of advancement of biologic aging (Fig 4-1). It is interesting to note that three important facial grooves, the nasolabial groove, labial groove, and mentolabial groove, are situated along important meridians that are part of the energetic network that, according to ancient, oriental medicine, runs through the body.1 The deepening of the nasolabial groove situated on the path of the meridian ruling vitality and opening to life testifies a loss of energy as the result of inner distress originating from emotional damage. The energetic losses marking the labial lines indicate inner rebellion and supressed revolt against destiny, whereas the mentolabial groove gathers the impacts of the “vessel of tears” located under the eyes, indicating an absence of self-defense and difficulty in communicating despair. Even if few can be convinced of the poetic significance of the progressive apparition of lines and wrinkles, these considerations are valuable in that they point out that a selective muscular activity takes place under the influence of specific psychologic states having effect when the environmental conditions cause aging or decay.2
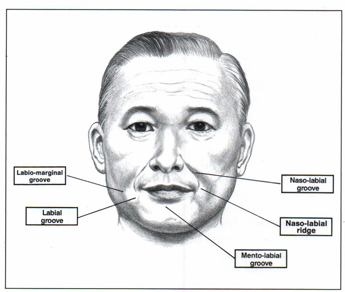
Fig 4-1 This sketch illustrates a limited number of facial grooves or sulcus surrounding the oral cavity that are associated with the nature of the individual tegumental relief or with the advancement of the biologic aging.
The anatomic changes that cause the appearance of aging take place early in life (Figs 4-2 and 4-3). Significant modifications are already apparent at the age of 25 years, with the descent of eyebrows, nasal tip, and chin vertex and the sinking of the nasal base. These movements accelerate abruptly at about 35 years of age under the influence of gravity, laxness, and thinning of the skin, which starts producing wrinkles and sulcus.3 Thin skin textures, generally exhibiting thin epidermis, lacking elastine, and with an irregular and scarce presence of collagen, are more susceptible to wrinkling, whereas thick skin textures with thick epidermis, abundant elastine, sebaceous glands, and collagen will prove more resistant to this deterioration. These statements should be modified depending on the influence that a number of elements, such as nutritional factors, way of life, and energetic potentialities, can exert. The original skin relief evolves and an undulating relief may become roughly marked, while a plump skin relief generally droops into folds, modifying the morphopsychologic significance exhibited by an individual. In mentioning the changes that can affect the osseous structures, the loss of skin and muscle elasticity, and the diminution of muscle strength inducing the progressive appearance of wrinkles, we have a concise image of this syndrome of decadence. This will inevitably affect psychic equilibrium when some event raises it to the level of consciousness.

Fig 4-2 Early perception of facial aging of muscular and tegumental origin characterized by the deepening of the nasolabial groove. (Courtesy of Dr U. Bürki, Geneva.)
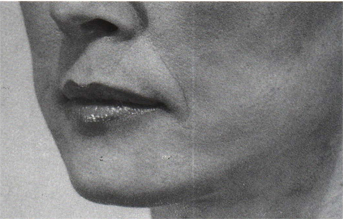
Fig 4-3 Successful effacement of the nasolabial groove and restoration of lip tonicity following rhytidectomy. (Courtesy of Dr U. Bürki, Geneva.)
In focusing our attention on the localization of facial aging, it is clear that it predominantly affects the lower one third of the face. Also, the basic anatomic facial grooves surround its receptor. This not only attests to the importance of the mouth but suggests its active participation in this phenomenon of deterioration to the point at which therapeutic action may sometimes compound the problem. Being familiar with the profound morphologic changes that affect the perioral structures and the lower one third of the face in a state of edentation, one can easily imagine from this extreme situation that the multitude and variety of intermediate states resulting from successive “accidental” traumas are capable of producing similar but attenuated consequences. Skeleton, muscle, ligaments, and teeth form a cohesive unit. Alteration to any part of it may affect regions far beyond those directly concerned.4 Pathologic situations materialized by the loss of teeth, migrations, tooth wear, faulty restorations, or tooth arrangements not only exhibit profound local morphologic changes, but these morphologic changes directly or indirectly influence the surrounding structures. This influence systematically affects facial muscles. Muscle collapse following tooth loss not only affects those muscles that have benefitted from this tooth support but also involves the collapse of associated muscles, which are connected by means of a network of fiber intrication (Figs 4-4 and 4-5).

Fig 4-4 Development of the nasolabial ridge underlined by the nasolabial groove and a deep labial groove.

Fig 4-5 Effacement of the nasolabial ridge and consequent diminution of the labial groove following full mouth rehabilitation.
Considering the alterations that can have an effect on the elements of the orofacial unit and their consequences, it seems that we are in the presence of a chain of reactions confirming the links existing between its constitutive elements.5,6 The diagrammatic representation of head posture maintenance demonstrates the close interdependence existing between these constitutive elements and reveals the collapse that may result from any accidental event (Figs 4-6 and 4-7).
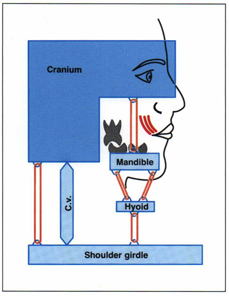
Fig 4-6 Diagrammatic representation of head posture maintenance and balance of craniomandibular muscles. The relaxation of facial muscles does not affect this equilibrium. (According to Sarnat.5)
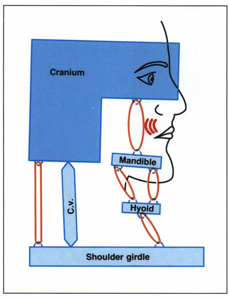
Fig 4-7 This diagram, simulating the loss of dental support, underlines its direct impact on the maintenance of facial musculature and the imbalance created on the whole craniomandibular system. (According to Sarnat.5)
Abnormal facial equilibrium, either morphologic or esthetic, can be ascribed to two major causes: (1) physiologic or programmed aging, generating changes in muscle and skin tonicity, and (2) pathologic aging, generated by accidental traumas affecting the oral cavity.
The difficulty consists of determining what in the facial appearance are the elements that result from oral pathologies and those that are a consequence of physiologic, programmed aging. This difficulty is greatly increased when it concerns individuals reaching an age at which this sequence of events may be considered normal.
The restoration of health and function of the oral organ will shed some light on these differences, with the restriction that there does not exist from one individual to another a chronology in the apparition of lines, sulcus, and wrinkles. A similarity of the effects resulting from a specific oral clinical situation, as a result of the variety of muscle fiber intrication and the nature of the original tegumental relief, is highly unusual.
The differential diagnosis seems somewhat easier when lip design comes into consideration. Lip design, which according to the morphopsychologic concept, results from the influence stemming from cerebral, sentimental, and instinctive action, depends upon its dentoalveolar support with which it is ultimately connected. It is also linked with the strength and tonicity of its muscular support. Any alteration affecting the dentoalveolar support will have a direct influence on facial musculature. From clinical practice we have observed that a protrusive outward roll of the upper and lower lip originating in a loss of skin and muscle tonicity takes part in the development of facial sagging (Figs 4-8 to 4-10). A loss of the vertical dimension of the lower facial one third affecting the strength and the extent of the working length of the infraorbital musculature, predominantly the quadratus labii superioris and zygomaticus, induces a muscle collapse. When this loss is illustrated by anterior tooth wear or lack of dentoalveolar support, an inward roll of the upper lip margin toward the corners can be observed. In case of anterior tooth migration affecting lip movements, a large variety of lip postures can take place (Figs 4-11 to 4-16). Functional disturbances naturally reflect on facial appearance, attesting to the link existing between function and esthetics. Although esthetic dentistry must take into consideration the interdependence existing among the elements constituting the oral environment, clinicians in esthetic dentistry and esthetic medicine should be aware of the effects of oral pathologies on premature aging of the face. This clearly calls for closer cooperation between these two specialties (Figs 4-17 to 4-19).
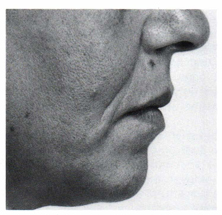
Fig 4-8 Muscle and tegumental laxness affecting the oral environment, producing a characteristic outward roll or redundancy of the upper and lower lips and deepening the nasolabial groove. (Courtesy of Dr U. Bürki, Geneva.)
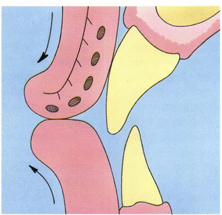
Fig 4-9 Schematic illustration of the outward roll of the lip. Its muscular and tegumental origin can be determined when tooth support is unaffected.
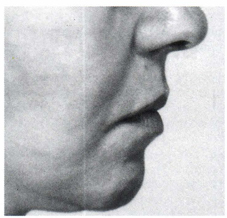
Fig 4-10 Restoration of tegumental and muscle tonicity and the restoration of lip design after rhytidectomy. (Courtesy of Dr U. Bürki, Geneva.)

Fig 4-11 Effacement of lip design with marked inward roll of the lip margin toward the corners. Deepening of the mentolabial groove. Vertical wrinkles underline the lower lip.
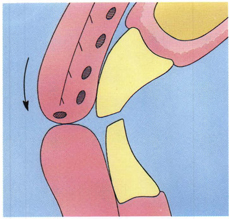
Fig 4-12 Schematic illustration of the inward roll of lip margin whenever a vertical reduction of tooth support takes place.
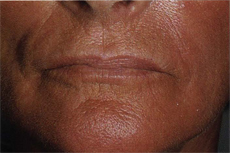
Fig 4-13 A frontal view illustrates the pathology affecting lip design and evidences the presence of a nasolabial ridge, predominantly on the right side, underlined by a labial groove.

Fig 4-14 Following rehabilitation, restoration of lip design with diminution of the mentolabial groove. Perioral structures regained strength as confirmed by the diminution of the vertical wrinkles surrounding the lower lip.
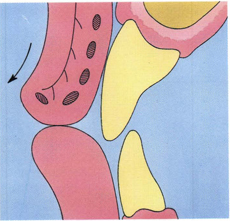
Fig 4-15 Schematic illustration of the closed lip posture when normal occlusal, muscular, and tegumental conditions exist. Typically, the incisal third of the maxillary incisor does not contact the inner part of the upper lip.

Fig 4-16 Restoration by means of fixed partial denture ending at the second premolar favoring abnormal contraction of the buccinator did not permit the total effacement of the nasolabial ridge, but this frontal view confirms the restoration of lip design.

Fig 4-17 Impressive image of facial decadence, exhibiting an important nasolabial ridge surrounded by unesthetic labial and nasolabial grooves. Lip design is distorted and the corners of the mouth depressed. (Courtesy of Dr U. Bürki, Geneva.)

Fig 4-18 After rhytidectomy the mouth design still looks unattractive and unnatural. An upper lip design presenting an inward roll toward the corners of the mouth can be considered a specific manifestation of oral pathologies. In this case, the competence of the surgeon has fortunately resulted in an avoidance of excessive tegumental pull. (Courtesy of Dr U. Bürki, Geneva.)
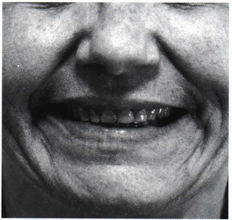
Fig 4-19 The picture of the smile showing a marked reduction of the tooth length confirms the expected pathologic oral situation. It indicates that the correction of specific facial deformities are within the competence of the dental profession. (Courtesy of Dr U. Bürki, Geneva.)
Tooth visibility
The amount of tooth exposure when lips and lower jaw are at rest is, like body posture, a muscle-determined position. This has been generally disregarded as an element of esthetic appraisal, if not totally ignored by the restorative dentist. For the prosthodontist, the determination of the incisal edge–lip length relationship was mainly based on clinical experience or on phonetic values, assuming that this should automatically achieve the correct position of the maxillary anterior incisor in the vertical plane.
An interesting study related to tooth exposure according to gender, racial factors, age, and lip length7 elucidated the extreme variability of this factor.
Tooth exposure showed an increase from blacks to Asians and whites for the maxillary central incisor and a decrease for the mandibular central incisor from Asians to blacks and whites (Fig 4-20).
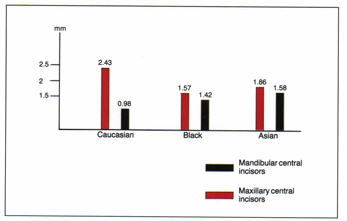
Fig 4-20 Diagram of exposure of maxillary and mandibular central incisors related to racial factor. (From Vig and Brundo.7)
Tooth exposure according to gender appeared to be significantly more important for females than for males because an average exposure of 1.91 mm was stated for males, whereas females had nearly twice as much tooth exposure (3.40 mm) of the maxillary central incisor, yet a minimal amount of 0.5 mm of mandibular incisor exposure. This suggests that treating patients using the same therapeutic values in this matter is an error that increases in importance when considering the parameters of lip length and age.
Age
The study evidenced a significant decrease of maxillary tooth length exposure relative to age, predominantly between the age of 30 and 40 years and a proportionate increase of mandibular incisor exposure, a situation that is esthetically, unanimously rejected (Figs 4-21 to 4-25).
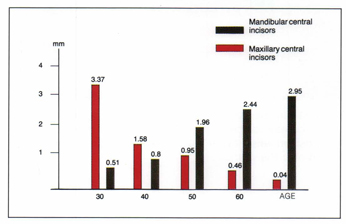
Fig 4-21 Diagram of exposure of maxillary and mandibular central incisors related to age. (From Vig and Brundo.7)

Fig 4-22 Average tooth exposure of a man in his 20s with natural dentition in slight mouth opening.

Fig 4-23 Facial sagging starts to proceed insidiously between 35 and 40 years of age. Slight mouth opening begins to display mandibular dentition as well.

Fig 4-24 In the 60s the maintenance of a healthy dentition does not assure the esthetic appearance of the dentofacial composition when facial muscle tonicity has not been maintained over the years.

Fig 4-25 At 70 years of age and in absence of oral pathologies, face sagging has proceeded so far that the restoration of an esthetic appearance is not affected by dental therapies and muscle retraining techniqes.
Table 4-1 shows that people with short upper lips expose the maximum maxillary incisor texture, whereas people with long upper lips expose predominantly lower anterior incisors.
| Table 4-1 Lip length | ||
| Lip length (mm) | Exposure of maxillary vertical incisor | Exposure of mandibular central incisor |
| 10-15 | 3.92 | 0.64 |
| 16-20 | 3.44 | 0.77 |
| 21-25 | 2.18 | 0.98 |
| 26-30 | 0.93 | 1.95 |
| 31-36 | 0.25 | 2.25 |
The assumption that tooth exposure is mainly of muscular origin influenced our decision to adopt the muscle retraining techniques as part of a maintenance program, preventing the sagging of the face at as early an age as possible.
Maxillary incisor visibility is an important parameter in esthetic appraisal because its decrease contributes to the early perception of aging of individuals in their 40s.
In selected clinical situations in which face sagging has proceeded too far and muscle retraining techniques become illusory, tooth anatomy must be elongated to fulfill rejuvenation’s requirements. This approach is only possible when it does not conflict with either functional problems or esthetic factors (Figs 4-26 to 4-28).

Fig 4-26 Pathologic clinical situation affecting an individual in her 70s, exhibiting periodontal and occlusal breakdown.

Fig 4-27 Whenever tolerated by the length of the lip line, the restoration of health, function, and esthetics implies a drastic increase of tooth length, such as that illustrated by this long-term provisional acrylic resin stabilization, following initial periodontal treatment.
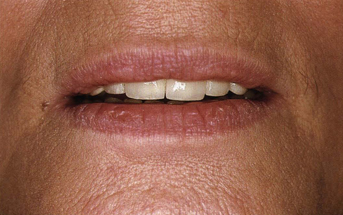
Fig 4-28 As a result, tooth display masks chronologic age but conforms to the advancement of the biologic age illustrated by the quality of skin texture. The nature of the tegumental relief enhances this rejuvenated image.
Components of the smile
The smile, which represents the most primitive form and the essence of human communicative ability, appears early in life in young children. Smiles and later facial expressions express transient feelings and emotions. A pleasant smile may produce an aura that enhances the beauty of the face as it pertains to the qualities and virtues of the human personality.
The perception of these qualities engenders the “attractive power,” a necessary vector to success in today’s world.
The individual’s ability to exhibit a pleasing smile directly depends upon the quality of the dental and gingival elements that it contains, their conformity to the rules of structural beauty, the relations existing between teeth and lips during smile, and its harmonious integration in the facial composition.
While the modalities of the development of facial expressions have been focused on by some authors,2,8–10 the esthetic lip–tooth relationships existing when smiling have been the object of surprisingly little investigation,11–15 as if the elements determining a favorable or negative connotation were unanimously recognized.
Rather than assuming what is of esthetic importance in the lip–tooth relationship during a smile, one should focus attention on the elements that receive esthetic approval16 and analyze them in the light of fundamental esthetic principles.
Lip line
The amount of tooth exposure during a smile depends on a variety of factors, such as the degree of contraction of the muscles of expression, soft tissue level, skeletal particularities, and the design of restorative elements, tooth shape, or tooth wear. Dentistry has arbitrarily classified three types of smiles that, relating the height of the upper lip relative to the maxillary anterior central incisors, are referred to as presenting a low lip line, middle lip line, or high lip line (Figs 4-29 to 4-32). While low lip line can sometimes become a cover for poor dentistry, the high lip line displaying a large amount of gingival tissue, reflecting aggressivity, affects those individuals exhibiting some type of maxillary protrusion or having a strong infraorbital facial musculature. The modalities for treatment of the high lip line are limited. Orthognathic surgery is disproportionate to the clinical situation. Orthodontic intrusion or surgical tooth lengthening with subsequent crown length reduction that may appeal to the esthetically concerned dentist could be of real help when the indications for this type of treatment really do exist. Muscle retraining techniques are often illusory as they are not able to provide a diminution of the strength of contraction of the infraorbital musculature. Surgical procedures carried out on the implicated facial muscles are most disappointing in their results. The ideal lip line seems to be obtained when the upper lip in reference to the maxillary incisors reaches the interdental gingival margin when smiling, a situation that is common to a large number of people.

Fig 4-29 High lip line in smiling displays teeth and gingiva.

Fig 4-30 Middle lip line displaying teeth and marginal interdental papillae when smiling.

Fig 4-31 Low lip line displaying a limited part of tooth anatomy when smiling.

Fig 4-32 Anterior low lip line with gingival posterior display.
Smile line
The smile line appears to be one of the most important factors contributing to a pleasant connotation of a smile. The smile line can be defined as a hypothetical curved line drawn along the edges of the four anterior maxillary teeth that has to coincide or run parallel with the curvature of the inner border of the lower lip. This situation, always favorably regarded, confirms the effect that cohesive forces can exert in any type of composition.
Observations may show that the degree of curvature of the incisal line is more pronounced for women than for men (Figs 4-33 and 4-34). A reverse incisal line or an abnormal lower lip posture, in effacing the elements that enable the perception of these cohesive forces, deeply affects the degree of attractiveness of the smile.

Fig 4-33 Feminine type of smile line characterized by the curvature of the incisal line that coincides with that of the lower lip.

Fig 4-34 Masculine type of smile line showing a straighter incisal line and producing a stronger morphopsychologic impact.
Upper lip curvature
In smiling, the position of the upper lip height relative to the teeth has been ideally located at the gingival margin of the maxillary central incisors and appears as an important factor of attractiveness (Figs 4-35 to 4-38).

Fig 4-35 In smiling, the curvature of the upper lip may be directed upward.

Fig 4-36 The specific strength of the muscles involved in the smile may produce a lateral stretch of the corners of the mouth.

Fig 4-37 A slightly downward curvature of the upper lip may occasionally be seen.

Fig 4-38 A pronounced downward curvature of the upper lip in smiling is not unusual.
The upper lip curvature that is expected to run upward from this central position to the corners of the mouth, depending on the sequence and degree of implication of facial muscles in the development of smile, has been found to be straight and even downward in a certain number of people, affecting the attractiveness of these smiles. In this type of situation some improvement can be obtained using muscle retraining techniques when the other components of smile do not compensate for this deficiency.
Negative space
Negative space can be described as the dark space that appears between the jaws during laughter and mouth opening. This dark space contributes to the individualization of the dental composition that is projected by color contrast. A similar dark space appears between the outer surface of the maxillary teeth and the corner of the mouth in smiling (Figs 4-39 and 4-40). These lateral negative spaces that result from the difference existing between the width of the maxillary arch and the breadth of the smile have been described to be in golden proportion with the anterior smiling segment.15 An adequate restoration of the lateral negative spaces will permit the characterization of the smile in conformity with the individual’s personality.

Fig 4-39 The presence of a lateral negative space may be considered a prerequisite of dentofacial esthetics, giving depth and mystery to the smile.

Fig 4-40 The absence of a negative space usually appraised by the public reflects exuberance and brilliance but indicates occlusal disturbances or inadequate restorative dentistry.
The importance of this space must be stressed even if it escapes the attention of the public because it not only represents a key factor in the harmony of the smile itself but also a factor of the harmonious proportionate relationship between the smile and other facial features. This indicates that some fundamental esthetic principles or their distortion are more easily perceived than others.
Smile symmetry
The implication of this important esthetic element in a pleasant connotation of smile refers to the relative symmetric placement of the corners of the mouth in the vertical plane (Figs 4-41 and 4-42). Symmetry can only be perceived in reference to a hypothetical central point or central midline. A close look at the nature of the symmetry of the dental composition determines the placement of this midline. A radiating type of dental symmetry draws this line automatically between the central incisors and contributes to the identification of the central contact line, whereas in a horizontal type of symmetry, the eye fixes on a central midline, the coincidence of which with the central interdental space does not assume any importance. When viewed from a distance the dental composition progressively loses its details and is perceived as a specific dental shape mimicking a horizontal type of symmetry on which the mind fixes a hypothetical midline in reference to facial parameters. Smile symmetry may be appreciated in the frame of the dentofacial or facial composition, depending upon the distance from which it is evaluated. In turn, facial midline or dental midline assumes the function of the central point.
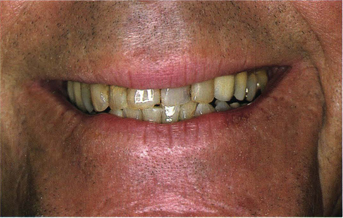
Fig 4-41 Smile symmetry refers to an identical placement of the corners of the mouth in the vertical plane of the face. It can hardly be evaluated at this distance of focus.

Fig 4-42 Smile asymmetry implies differences in the placement of the corners of the mouth in the vertical plane of the face. It is barely perceptible at this distance.
In viewing the dentofacial composition, the need for a coincidence between the commissural line and the line running from the tip of a cuspid to the other, which will be named occlusal line or occlusal plane, can be demonstrated (Fig 4-43). From a distance enabling the perception of the facial composition, observation will show the progressive importance of the parallelism of lines that must exist between the corners of the mouth or commissural line and the occlusal line (Fig 4-44). This infers that in smiling the placement of the corners of the mouth should conform to a succession of parallel lines, cohesive forces assuring the esthetic strength of the facial or dentofacial composition (Figs 4-45 to 4-48). The central midline, hypothetical or imposed by the nature of the elements constituting the facial or dentofacial composition, crosses this succession of lines, ensuring the presence of segregative forces, a prerequisite for esthetic appraisal. The esthetic evaluation of smile symmetry relies on the unconscious perception of the involved crossing joint.

Fig 4-43 In this dentofacial composition, the evaluation of the symmetric placement of the corners of the mouth in the vertical plane can only be done with reference to the coincidence of the commissural and occlusal lines. Note that asymmetric right and left anterior dental segments around the central midline can be observed (see Fig 4-56).
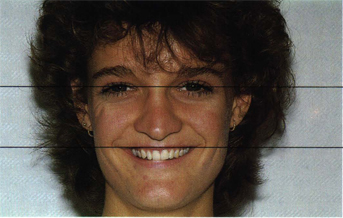
Fig 4-44 When attention is focused on the facial composition, the coincidence of commissural and pupillary lines becomes a prerequisite for the esthetic appraisal of the smile that seems unaffected by the asymmetry exhibited by the right and left anterior dental segments in the horizontal plane.
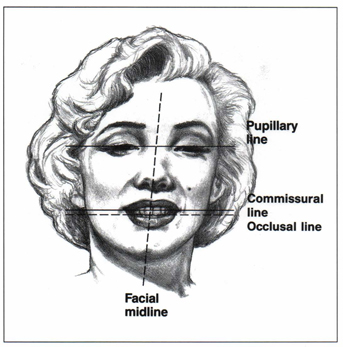
Fig 4-45 Illustration of the coincidence of pupillary and commissural lines, prerequisite requirements of smile attractiveness at this distance of focus. Smile and facial components must be evaluated by reference to facial factors.
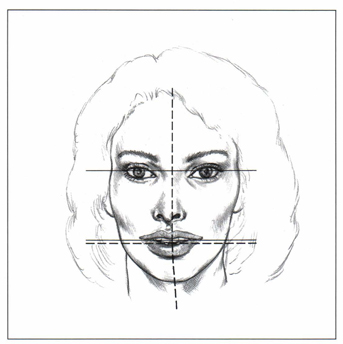
Fig 4-46 The esthetic integration of the smile in the facial composition appears unaffected by the directional variation of the facial midline but requires the presence of cohesive forces, illustrated by the coincidence of pupillary and commissural lines and subsequently by that of the occlusal line.
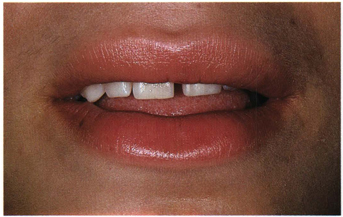
Fig 4-47 At first glance this noncoincidence of commissural and occlusal lines results from tongue parafunctional interference. A more precise examination of the facial composition evidences noncoordinate retraction and elevation of the mouth corners during the smile process, leaving the left side of the mouth in a lower position. The dental composition illustrates a type of individual dominance. (See Figs 1-53 and 1-54.)
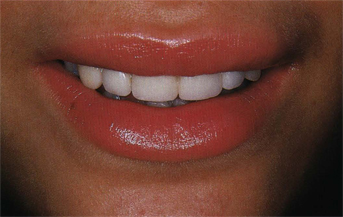
Fig 4-48 Treatment techniques have focused on the control of the parafunctional tongue habits and on a coordinated muscular development of the smile. Restoration was carried out taking into consideration the restoration of line coincidence to ensure esthetic strength of the composition. After restoration, the dental composition exhibits a segmental dominance, stressed by the color change, reflecting segregative forces that approach a level of interference even if it conforms to the patient’s desires.
Occlusal line or occlusal frontal plane
In today’s dentistry our field of vision is restricted by the miniaturization of restorative procedures and is hampered by the use of protective material and by the constraints of our working position. For the majority of professionals the perception of lines is limited to those that are part of the dental composition (Figs 4-49 and 4-50). A noncoincidence of lines between the occlusal frontal line and the hypothetical gingival line running from the zenith of anterior teeth, usually from the right to the left canine, exhibiting an imbalance of shapes, should be perceived, but usually, the attention is focused on the occlusal line, delimiting the incisal silhouette and perceived by color contrast with the anterior negative space. This characteristic has been widely reproduced by magazines and underlined by caricaturists to the point that this image of a straight incisal line has been adopted by the public as a standard of dental esthetics. This stresses the differences existing between professional and public perception of the particularities of dental composition.

Fig 4-49 At a usual working distance, visual perception evaluates the coincidence or noncoincidence that may exist between the occlusal line and other hypothetical lines drawn in the oral cavity, cohesive forces assuring the esthetic strength of the composition. Attracted by segregative forces beyond the level of tolerance, this evaluation does not take place.
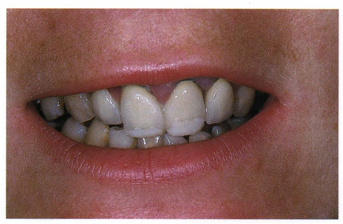
Fig 4-50 The visualization of the dentofacial composition reinforces the necessary coincidence of the occlusal and commissural lines. By reason of the substitution of the incisal line for the occlusal line this coincidence of lines is not perceived.
Instead of fighting against this distortion of reality, when restoring details of the anterior dental segment, one must understand and make understood that these differences of perception simply originate from different distances of focus. The observation will stress the fact that this occlusal line can be visualized as being part of the dental, dentofacial, and facial composition, which tends to explain the importance attributed to it. From the viewpoint of esthetic analysis, this occlusal line, underlined by the segregative forces of the negative space, takes part in a system of coinciding lines, cohesive forces, the multiplicity of which assures the esthetic strength of the composition (Figs 4-51 to 4-53). Whenever this system loses cohesion, careful examination may often evidence disturbances or pathologies showing the link between function and esthetic (Fig 4-54).

Fig 4-51 The restoration of the coincidence of the commissural and occlusal lines, cohesive forces of a composition, strengthens the composition. At any level of mouth opening or smile, this coincidence should be extended to the lower dental composition. Here muscle retraining techniques should help correct the still existing deficiencies.

Fig 4-52 Restoration of the coincidence of the occlusal and gingival lines, running along the zenith of the canine and lateral incisors. (Root bleaching has been limited to the marginal area.)
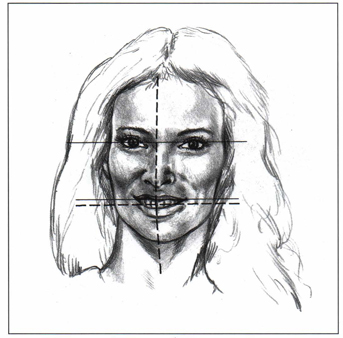
Fig 4-53 The esthetic connotation of a smile is usually seen as a succession of coincidental lines, cohesive forces characterizing the dental, dentofacial, and facial composition.
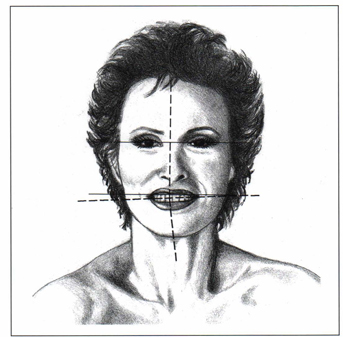
Fig 4-54 Whenever a divergence can be stated, not only is the esthetic strength of these cohesive forces greatly reduced but there is also evidence of a facial muscle or functional disturbance.
The perfect smile
According to these statements a perfect smile is characterized by a middle tooth–lip line relationship, an incisal line running against the upper border of the lower lip, and an upper lip presenting an upward curvature. The mouth corners are symmetrically aligned to the pupillary line and leave a proportionate bilateral negative space. When it contains and is surrounded by dental and facial elements that conform to fundamental esthetic principles, it may reach another level of appreciation if their harmonious integration into the individual’s morphopsychologic profile generates an emotional psychologic reaction.
Dental midline
The problem of the placement of the dental midline, an imaginary vertical line that separates the two central incisors and a prerequisite for the restoration of the anterior edentulous area, has been mentioned when dealing with smile symmetry. Nevertheless, some clarification seems necessary because the literature that deals with this question reveals a real division of thought. Recommendations include the following:
1. Place this midline precisely in the facial midline or in the middle of the mouth using the lingual papilla or the labial frenum as landmarks.17
2. Never establish it in the precise midline because it may contribute to an artificial appearance.18
Research has statistically demonstrated, using the lip philtrum as a reference guide, that the maxillary midline coincided precisely with the facial midline in 70% of cases and that esthetics was not compromised by a slight deviation from the central midline. The same study revealed that maxillary and mandibular midlines failed to coincide in 75% of cases. This definitely means that the lower midline should not be regarded as a reference for the placement of the maxillary midline19 when dealing with the restoration of the anterior edentulous areas.
Although a facial composition may give the general feeling of symmetry, it is well known that variations between both sides of the face exist, and when mirror images of one side are placed together, an entirely new face is created that tends to look artificial20 because the subtle differences in shape, lines, and color have been eliminated and with them the basic elements of sublimation that nature most often engenders. This may give credit to those who believe that a precise midline placement may contribute to an artificial appearance.
The use of anatomic landmarks, or more specifically, the incisive papilla can contribute to an initial evaluation of the placement of the dental midline, and the observation confirms the reliability of this initial placement. One should keep in mind that both facial and dental midlines are the necessary vectors that enable esthetic appraisal through the perception of the parameters of symmetry and balance. By reason of the differences existing between the right and left side of the face, the facial midline is far from providing a precise geometrical division.
This may explain the variables stated in the definition of this parameter:
1. Vertical line drawn through the forehead, nose columella, dental midline, and chin.21
2. Imaginary line that runs vertically from the nasion, subnasal point, interincisal point, and pogonion.22
Although both definitions include the coincidence of dental and facial midlines, the relationships of which have been suggested as having a definite influence on the harmony of the dental composition,23 one should point out that the visualization of this coincidence, requiring various degrees of smile or mouth opening, is only hypothetical, keeping in mind that the dental midline can hardly be perceived at the distance from which facial composition can be evaluated.
Part of the dentofacial composition, the dental midline, is best visualized in the dynamics of the smile. It should logically be placed in its center. It is important that the coincidence of the dental midline with the precise midline of the smile be determined by the nature of the symmetry exhibited by the dental composition. An anterior diastema or a marked radiating symmetry determines the placement of this midline, tending to induce visual tension when placed off the center of the smile unless equilibrium required by the phenomenon of balance is affected by the visualization of equal right and left dental segments (Figs 4-55 and 4-56). This explains why when placed off the precise center of the philtrum, the dental midline does not often induce visual tension.

Fig 4-55 A large diastema establishes a strong central midline, the location of which in the center of the smile is needed to avoid visual tension. Esthetic appraisal is evaluated according to the principle of symmetry.
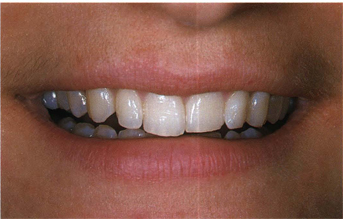
Fig 4-56 When the central midline does not coincide with the center of the smile, esthetic equilibrium may be achieved by the balance of lines, of size and the amount of light reflecting from the right and left anterior segments. It can be observed how the lower lip stresses the position of the hypothetical midline.
What becomes important is the fact that the predominant cohesive forces, commissural, occlusal, and pupillary lines determine the perpendicular direction of segregative forces, precisely illustrated by the dental midline and the dental elements related to it. Deviations affecting these elements can hardly be compensated for by the phenomenon of balance and will create strong visual tension (Figs 4-57 and 4-58).

Fig 4-57 Both central incisors diverge from hypothetical midline drawn perpendicular to the commissural line, inducing imbalance of the lines. This factor generates esthetic reproval.

Fig 4-58 This improvement of axial line equilibrium, by shortening the left lateral incisor and lengthening the right central incisor, took place during esthetic evaluation. It restored the axial direction of the central midline.
Golden rules
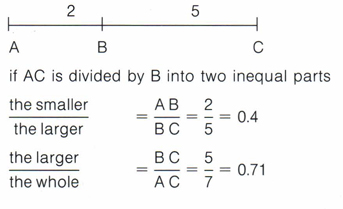
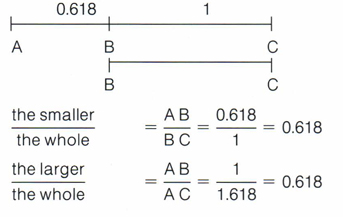
The definition of the laws of beauty and harmony has been a constant preoccupation of Greek philosophers and mathematicians. The connection of beauty with numerical values conforms to the philosophy that beauty always appears as fundamentally exact. The finding of an intriguing relationship in the harmony between two parts, which can be described as follows, has been attributed to Pythagoras: The smaller to the larger is equal to the sum of the whole related to the larger (Fig 4-59).
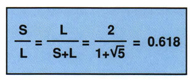
Fig 4-59 Mathematical formula of the golden proportion.
Ever since its formulation in antiquity, this number, called the “golden number” or “golden section,” has attracted the attention of mystics, artists, and scientists. Johannes Keppler (1611) saw in this golden section “an idea used by the Creator to generate the similar from the similar,” and its esthetical value was stressed by Luca Pacioli24 in his book Divine Proportione (1509) illustrated by Leonardo da Vinci. The extension of the study of the golden number from its linear form to the surface form is attributed to Hambridge,25 and more recently Le Corbusier26 developed a scale based on the golden proportions of the human body that he intended to integrate in a dimensional living space in accordance with its movements and positions. Harmony in proportion has been defined as an esthetic principle, part of the essential beauty. When considering the size and design of natural elements,27 we must always keep proportion in mind because this golden relationship has been demonstrated in organic forms of nature and in animal and human forms.28,29
The reason that elements perceived through the division of this golden number are different from any other proportion, and what these differences are, have been demonstrated mathematically.
The results of these equations are different, whereas the results of the equations that use the golden number as surface or line division are equal.
This tends to prove mathematically that any line divided in the golden proportion is in equilibrium around the point of division.
Linear progressions and surface division by this same number are common in nature30 both geometrically and arithmetically.
Geometric progressions can be obtained by multiplying each term by 1.618 or dividing by 0.618:
| 1.000 × 1.618 = 1.618 | 1.000/0.618 = 1.618 |
| 1.618 × 1.618 = 2.618 | 1.618/0.618 = 2.618 |
| 2.618 × 1.618 = 4.236 | 2.618/0.618 = 4.236 |
In the arithmetic progression each term is the sum of the preceding two terms:
| 0.618 + 1.000 = 1.618 |
| 1.000 + 1.618 = 2.618 |
| 1.618 + 2.618 = 4.236 |
It can therefore be stated that the progression using the golden number is unique because three different methods produced the same result.
This mathematical concept can be applied to geometrical calculations with real satisfaction. However, its strict and unsophisticated application to organic figures is not evident and the concurrence is never perfect. This explains why some considered it necessary to distinguish between “constructive systems” acting in graphic designs and “objective systems” in regard to living forms.31 Philosophically, it seems easier to consider that this numerical value simply tends to point out a quality of information for esthetic appraisal. Yet, studies and experiments32 have amply demonstrated that this surface division, sensed by the eye, independently from ethnic or civilization factors, creates an esthetic appeal.
Our attention must be focused not only on the simple manifestations of this golden section but on the subtle and fascinating variations that nature exhibits (Figs 4-60 and 4-61/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


