Chapter 4
Perception is Reality
Meeting patients’ expectations is an essential link in the service-profit chain. When a new patient arrives at your practice, she or he will have prior expectations. These may relate to the way they are greeted, the environment, the range of services you provide, the fees and the way they are treated. As they approach your premises, those expectations are in a state of flux influenced by everything going on around them. This engagement of the senses is what perception is about and it helps to create the reality in the patient’s mind and it plays an important part in remodelling expectation.
But, it is not always as easy as it sounds. The reason is that perception is affected by so many variables and they can be different for different people. And when they are the same, different people attach different value to them.
As Colin Cherry puts it in On Human Communication:
“though many different pairs of people may say ‘the same thing’ (linguistically) on different occasions in conversation, each occasion, as an event, is observably different in many aspects from the others; such differences depend upon people’s accents, their past experiences, their present states of mind, the environment, the future consequences of interpreting the message, knowledge of each other, and many other factors …”
Whether we like it or not, we have all been conditioned to interpret visual images in certain ways. For example, if food on a plate looks attractive, then the association is that it must taste good. There are few absolute truths – it is all down to what you see and what conclusions you draw from what you see.
The Psychology of Perception
The science behind managing the perception is psychology. “Spin doctoring” is the popular term to describe the work of those who apply the psychology of human perceptions in their work. It is a sophisticated form of marketing. It is a great pity that a valuable tool has achieved notoriety because of the way it has come to be used. “Spin doctor, heal thyself” would not be inappropriate advice to the industry. For this reason, the word is used with caution and relates to the psychology of perception – not its perceived meaning. The irony will not be lost on readers.
To be effective, spin has to be invisible. Timothy Bewes, author of Cynicism and Postmodernity, writes: “the moment when we become aware of the existence of spin is the moment of its disappearance. Effective spin requires a general unawareness of its existence.” The power of positive perceptions underpins word-of-mouth marketing; it leads to recommendations and helps to build successful businesses.
Your Professional Image
How we look, dress, act and speak all contribute to our image. Psychologists refer to it as pattern recognition – we “template match”. When new patients enter your practice, they template match from the moment of arrival. Ask yourself the question: does your practice image reflect the typical template or there is something about it that makes you different? Is there anything you could do to break the mould and alter the perception – something akin to the “wow!” factor?
The Greek philosopher Epictetus probably never thought of himself as a spin doctor. He was, however, acutely aware of the psychology of perception. He taught his pupils “first to know who you are, then adorn yourself accordingly”. So, before you look at your practice, look at yourself.
Self-image is where it starts. Dimbleby and Burton in their book More Than Words proposed the model shown in Fig 4-1. There is a relationship between self-image and self-esteem. The more positive one’s self-image, the higher one’s self-esteem. Self-image is connected also with communication performance. For example, if we believe we are ugly, we may expect to be rejected. We may as a result enter into communication expecting rejection and thus present ourselves in a way, which actually invites rejection – the so-called self-fulfilling prophecy. We are also likely to seek from others confirmation that our self-image is accurate. Thus, if we see ourselves as winners, so will others and, as a result we may well turn out to be winners; if we see ourselves as losers, then losers is what we may become.
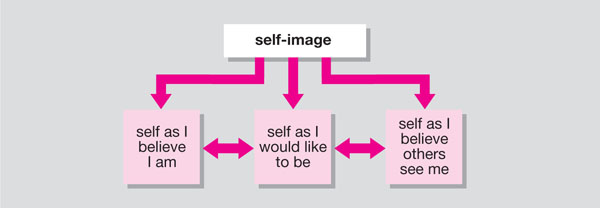
Fig 4-1 Self-image and self-esteem.
Anecdotal evidence suggests that many dentists do not relish the thought of discussing costs of treatment. Many writers in the field of practice management describe a phenomenon where the brain suggests the correct fee for a procedure but the mouth utters a lesser one – the so-called oro-fiscal drag! (In fact, my co-author refers to it in Chapter 7.) This observation is based partly on fear of rejection and any communication with patients on the subject could turn out to be a self-fulfilling prophecy.
Choice of clothing can also affect the patient’s perception. Clothing influences first impressions. The white coat has become a symbol of the health professional, but these conventions are not as rigid as they once were. Style and cleanliness in clothing may be more important and indicate adherence to traditional values of hygiene and sterility.
So who is going to take responsibility for your image? Only you can and you must. It is an essential discipline in all aspects of the business of dentistry, including clinical dentistry. Self-monitoring is the term that has been coined by psychologists to express the extent to which a person notices the self-presentation of others and uses that information to guide their own self-presentation. People who score highly on their ability to self-monitor are better able to change their behaviour to suit the situation or audience – and are known to perform better.
The Halo and Horn Effects
The assumptions that we make are known as the “halo effect”. This has been defined as bias created by an observer’s tendency to rate, perhaps unintentionally, certain objects or persons in a manner that reflects what was previously anticipated. For example, people with glasses and high foreheads are frequently thought of as intelligent – even if we may not have direct evidence of this. The “horn effect“ refers to the same phenomenon, but relates to undesirable characteristics. Anecdotal evidence suggests that we frequently judge (or rather misjudge) our patients in this way, making assumptions about their ability to afford treatment and their motivation, without having the evidence. By being aware of the tendency, it is possible to override it.
The Weighted Averaging Effect
We know that our judgements of other people are weighted averages of the information we have about them. In reaching decisions about our patients and their personalities and motivation towards dental health, we tend to take everything we know about them, but give some information a greater weight, and then produce an average of the information we have. Negative information will generally be given more weight than positive information. The same process takes place when patients look at us – they make the same weighted judgement errors.
The “Primacy” Effect
The “primacy” effect is a psychological term that means that when presented with a bunch of information, what we remember most often is that which entered the mind first. In other words, first impressions count. What could be more important in a patient-centred business? The primacy effect reflects the weighted average phenomenon: the information we obtain first is weighted more heavily than the rest because it is assumed to be more important.
The “Recency” Effect
It is also generally accepted, somewhat paradoxically, that if there is a significant time lag between the first piece of information and the next, then the last piece of information will carry more weight. This is known as the “recency” effect.
The notion of the primacy effect that “first impressions count” was challenged in a televised experiment carried out on the BBC Television programme Tomorrow’s World in March 1995. In this experiment viewers saw a young man being interviewed for a job as an ambulance driver. He began by saying that he had been in the army medical corps and gave some description of his experience there. He ended by saying that he had not stayed long in any job since leaving the army. This was broadcast in one part of the country. In another part, viewers saw the facts presented in reverse order, i.e. he stated first that he had not held any job long after leaving the army. In the latter broadcast 54% of viewers voted that he had made a favourable impression in comparison to only 45% in the first broadcast – which seems to suggest that last impressions count.
Stereotyping
Stereotypes are generalisations about what people in a particular group are like. The social identity theory has been very influential in European psychology and suggests that we need to create social maps, which we do by grouping, and then uphold values and traditions of our own groups relative to other groups. The groups can be defined on any number of criteria but the common ones are:
-
gender
-
race
-
occupation
-
age.
In general practice, patients tend to be identified within these broad categories but also within sub-categories according to the structure of the practice. Patients may be labelled as either NHS (further divided into fee-paying and exempt) or private, and associations are made between job status and affordability. The managing director is one stereotype – she or he must be well paid, able to afford private care, be highly motivated towards oral health, and so on. Psychologists have suggested there is a tendency for us all to lean towards stereotyping, so we must learn to inhibit the “automatically activated stereotype” to become non-prejudicial.
We must remember that patients also display stereotype tendencies towards dentists. If the perceptions are negative (as they often are), the real challenge is to break the stereotype mould – but that is not easily done. Consider a typical remark made by a patient and one that many dentists have heard on numerous occasions in one form or another: “I hope I do not have to see you again too soon. I do not know why I say that. You have never hurt me, but you know what I mean.” The patient is recalling information that is consistent with their pre-existing stereotype rather than information that is not consistent – as evidenced by the comment “I do not know why I say that. You have never hurt me.” It can take time to change the image of the stereotype that is “the dentist” and one way to go about it is to borrow some ideas from the image-makers and the brand creators.
Branding
The concept of branding has become relevant in the business of dentistry because of new entrants into the business. Many of the dental bodies corporate are branded and are aware that branding makes a difference to the way people make choices about products and services. James Hul/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


