Carbohydrate
The Efficient Fuel
• Identify major carbohydrates in foods and in the body.
• Outline ways glucose can be used by the body.
• Summarize the functions of dietary carbohydrates.
• Explain the importance of dietary carbohydrates.
• Identify dietary sources of lactose, other sugars, and starches.
• Summarize the role and sources of dietary fiber.
• Describe the role of carbohydrates in the caries process.
• Formulate recommendations for patients concerning carbohydrate consumption to reduce risk for dental caries.
 Test Your NQ
Test Your NQ
1. T/F Raw sugar is nutritionally superior to white sugar.
2. T/F Fructose is the principal carbohydrate in honey.
3. T/F All caloric sugars can be metabolized by plaque biofilm.
4. T/F The desire for sweetness in the diet is an acquired taste.
5. T/F Fiber tends to regulate the rate of foods passing through the gastrointestinal tract.
6. T/F Carbohydrates are absorbed as monosaccharides.
7. T/F Excessive consumption of carbohydrates is the main cause of obesity.
8. T/F Glucose is the same as table sugar.
9. T/F Eliminating sucrose from the diet prevents development of dental caries.
10. T/F Natural sugars in foods can be just as cariogenic as added sugars.
Carbohydrates have been the major source of energy for people since the dawn of history. Worldwide, carbohydrates are the most important source of energy, furnishing 80% to 90% of kilocalories for some African and Asian nations. Nutrition experts from many countries recommend that carbohydrates should represent 50% of total energy intake,1 yet only 40% to 50% of the American diet is from carbohydrates.2 Carbohydrate foods add variety and palatability to the diet and are the most economical form of energy.
As discussed in Chapter 2, carbohydrates contain carbon, hydrogen, and oxygen. During photosynthesis, carbon dioxide and water result in formation of carbohydrates and the release of oxygen. Because glucose and other carbohydrates are essentially hydrogen (and oxygen) atoms bound to a carbon backbone, a carbohydrate could also be referred to as a “hydrated carbon.” The popular belief that carbohydrates have some mysterious “fattening” power is unfounded. During the 1950s, carbohydrates acquired a bad reputation in the United States as best-selling books claimed Americans were victims of “carbohydrate poisoning.” More recently, critics have labeled sugar as “toxic” and “addictive.” Naturally, these unscientific statements affect food consumption patterns. Resurgence of the popular low-carbohydrate, high-protein, weight-reduction diets have caused the pendulum to again swing away from choosing carbohydrate foods. Many of these diets are nutritionally unbalanced, providing inadequate amounts of nutrients known to help protect against several chronic diseases.
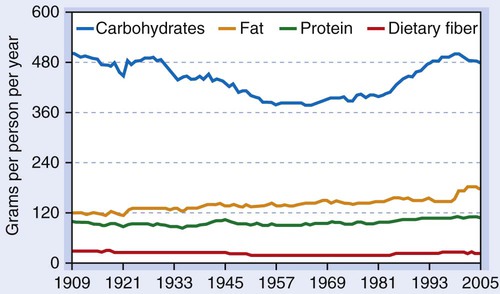
As can be seen in Fig. 4-1, carbohydrate intake has fluctuated more than intake of any other macronutrient. In 1977, the U.S. Senate Select Committee on Nutrition and Human Needs released Dietary Goals for the United States, advising Americans of reduced risk of various chronic diseases by consuming more complex carbohydrates (fruits, vegetables, legumes, and whole-grain products). Food supply data indicate that 49% of total kilocalories come from carbohydrates for men, and 51.6% for women. Americans consume less than eight servings of grain products daily and less than one serving of whole grains.3 Even if people are consuming an adequate number of servings from the whole grains and refined grains group, the types of foods chosen need to be adjusted to improve fiber intake and decrease added sugars (sugars added to foods during processing or at the table). Because most high-carbohydrate food choices are regular sodas, cakes, cookies, pastries, and pies, intake of fat and sugar is detrimentally affected. Mean intakes of caloric sweeteners decreased from 100.1 g per day in 1999-2000 to 76.7 g per day in 2007-2008.4
Classification
Chapter 2 and the Evolve website provide detailed biochemistry information regarding carbohydrates, including their structure and metabolism. Generally, the chemical components of carbohydrates are in these proportions: Cn(H2O)n. An empirical formula such as C6H12O6 or C12H22O11 can readily be identified as a carbohydrate. The number of carbon atoms in the molecule is used to classify carbohydrates. Monosaccharides are simple sugars containing two to six carbon atoms. Disaccharides are composed of two simple sugars joined together and contain 12 carbon atoms. Polysaccharides are complex carbohydrates containing a minimum of 10 units of various simple sugars.
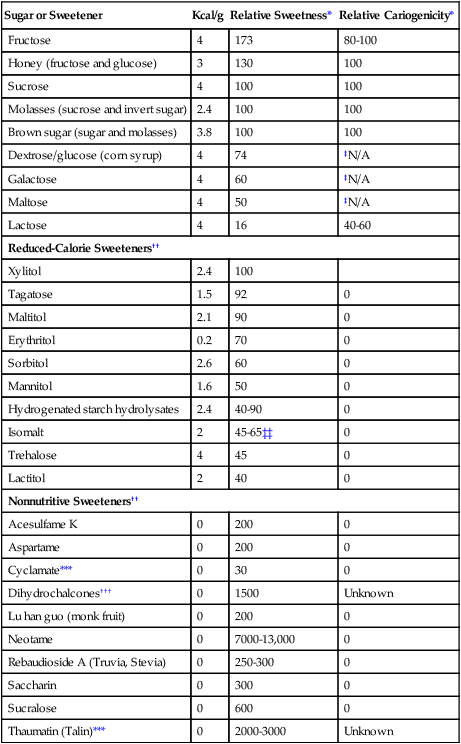
Monosaccharides and disaccharides contribute to the palatability of a food because of their sweetness. Temperature, pH, and the presence of other substances influence the sweetness of a food. Relative sweetness of sugars is measured by subjective sensory tasting; sucrose is used as the standard of comparison (Table 4-1).
Table 4-1
Sugars and sweeteners: caloric value, relative sweetness, and cariogenicity
| Sugar or Sweetener | Kcal/g | Relative Sweetness* | Relative Cariogenicity* |
| Fructose | 4 | 173 | 80-100 |
| Honey (fructose and glucose) | 3 | 130 | 100 |
| Sucrose | 4 | 100 | 100 |
| Molasses (sucrose and invert sugar) | 2.4 | 100 | 100 |
| Brown sugar (sugar and molasses) | 3.8 | 100 | 100 |
| Dextrose/glucose (corn syrup) | 4 | 74 | ‡N/A |
| Galactose | 4 | 60 | ‡N/A |
| Maltose | 4 | 50 | ‡N/A |
| Lactose | 4 | 16 | 40-60 |
| Reduced-Calorie Sweeteners†† | |||
| Xylitol | 2.4 | 100 | |
| Tagatose | 1.5 | 92 | 0 |
| Maltitol | 2.1 | 90 | 0 |
| Erythritol | 0.2 | 70 | 0 |
| Sorbitol | 2.6 | 60 | 0 |
| Mannitol | 1.6 | 50 | 0 |
| Hydrogenated starch hydrolysates | 2.4 | 40-90 | 0 |
| Isomalt | 2 | 45-65‡‡ | 0 |
| Trehalose | 4 | 45 | 0 |
| Lactitol | 2 | 40 | 0 |
| Nonnutritive Sweeteners†† | |||
| Acesulfame K | 0 | 200 | 0 |
| Aspartame | 0 | 200 | 0 |
| Cyclamate*** | 0 | 30 | 0 |
| Dihydrochalcones††† | 0 | 1500 | Unknown |
| Lu han guo (monk fruit) | 0 | 200 | 0 |
| Neotame | 0 | 7000-13,000 | 0 |
| Rebaudioside A (Truvia, Stevia) | 0 | 250-300 | 0 |
| Saccharin | 0 | 300 | 0 |
| Sucralose | 0 | 600 | 0 |
| Thaumatin (Talin)*** | 0 | 2000-3000 | Unknown |
††Data from Calorie Control Council, Copyright © 2012 Calorie Control Council. Accessed August 16, 2013: http://www.caloriecontrol.org/.
‡‡Accessed August 16, 2013: http://toxnet.nlm.nih.gov/cgi-bin/sis/search/a?dbs+hsdb:@term+@DOCNO+7969
***Not approved for use in the United States; approved for use in the European Union and Zimbabwe.
†††Not approved for use in the United States; approved for use in Canada, European Union, and more than 100 other countries.
Monosaccharides
The simplest carbohydrates, monosaccharides, are absorbed without further digestion. The monosaccharides of greatest significance in foods and body metabolism are glucose, fructose, and galactose. Chapter 2, Fig. 2-3 identifies slight differences between these three six-carbon sugars and glucose.
Disaccharides
Sucrose
Granulated table sugar is the most common form of sucrose, which is a combination of one molecule of glucose and one molecule of fructose, as shown in Chapter 2, Fig. 2-5. Commercially, sucrose is produced from sugar cane or sugar beets (not to be confused with red beets). It is also found in molasses, maple syrup, and maple sugar. Some fruits (apricots, peaches, plums, raspberries, honeydew, cantaloupe) and vegetables (beets, carrots, parsnips, winter squash, peas, corn, sweet potatoes) naturally contain varying amounts of sucrose.
Maltose
Maltose, shown in Chapter 2, Fig. 2-4, contains two molecules of glucose. Also called malt sugar, maltose does not occur naturally. It is created in bread making and brewing beer and is present in some processed cereals and baby foods.
 Dental Considerations
Dental Considerations
• Assess patients with an increased risk of dental caries for frequency of sugar intake, including sources of natural and added sugars.
• Newborns exhibit a preference for sweetness, so it is not considered an acquired taste. Although infants and young children typically select the most intensely sweet tastes, the pleasure response to sweet taste is observed across individuals of all ages, races, and cultures.5
• A judgmental attitude or criticism by the dental hygienist is not beneficial in modifying a patient’s use of carbohydrates or sugars.
 Nutritional Directions
Nutritional Directions
• All caloric sugars and starches, whether they are naturally occurring in foods or added to foods, have some cariogenic effect.
• Sugar alcohols are not fermented alcohols and do not need to be restricted by individuals suffering with alcoholism.
• All disaccharides contain the same caloric and nutrient content. The body cannot distinguish between natural honey, refined table sugar, or high-fructose corn syrup (see Health Application 4); all are absorbed and metabolized in the same manner as their component sugars.
• Encourage use of hard candies and chewing gum containing sugar alcohols (xylitol and sorbitol) to prevent caries. However, inform patients that using more than three to four pieces of sugar alcohol–containing items daily may cause gastrointestinal distress.
Polysaccharides or Complex Carbohydrates
Complex carbohydrates, also called polysaccharides, contain more than 10 monosaccharides (see Chapter 2, Fig. 2-7). Some polysaccharides have a role in energy storage and are digestible. Dietary fiber is largely indigestible by intestinal enzymes in humans.
Starch
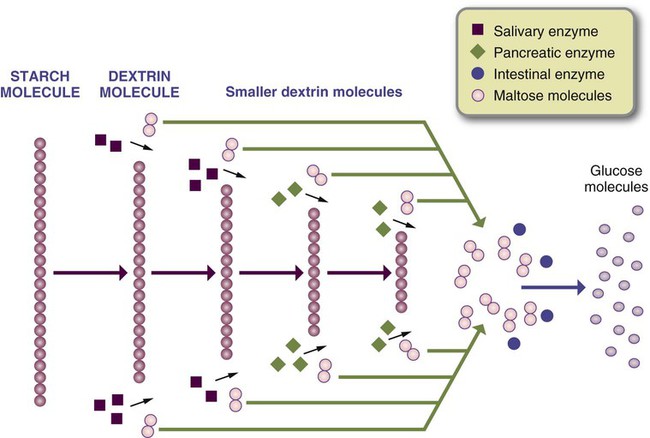
Starches are composed of many glucose units that may be in long chains or branched. Most food sources of complex carbohydrates are in the form of starch from cereal grains, roots, vegetables, and legumes. The amount of starch present in a vegetable increases with its maturity. For example, corn tastes much sweeter immediately after it is picked than it does several days later because the simple sugars in corn have not developed into starch. In contrast, the amount of starch in fruit decreases as it ripens—that is, complex carbohydrates are broken down during the ripening process into simple sugars. In digestion, complex carbohydrates are broken down into dextrin molecules until the end product, glucose, is absorbed (Fig. 4-2).
Glucose Polymers
Industrially-produced carbohydrate supplements are composed of glucose, maltose, and dextrins. Dextrins are long glucose chains split into shorter ones or intermediate products of digestive enzymes on starch molecules. In the process of toasting bread, dextrins are produced (see Fig. 4-2). Consistent with other carbohydrate products, glucose polymers provide energy equivalent to 4 kcal/g.
Glycogen
Glycogen is the carbohydrate storage form of energy in humans (see Fig. 2-7). Stored in the muscle and liver, glycogen is readily available as a source of glucose and energy. Carbohydrates are frequently consumed in excess of immediate energy needs. Excess glucose is converted to glycogen until the limited glycogen storage capacity is filled; simultaneously, glucose is converted into fats and stored as adipose tissue. The total amount of glycogen stores is relatively small, only enough to meet energy demands for less than a day.
Dietary Fiber
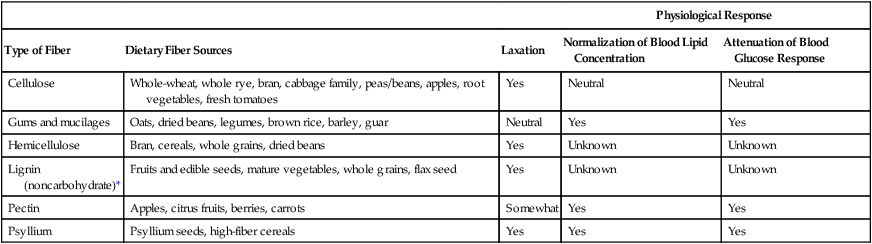
Dietary fiber includes polysaccharides, lignin, and associated substances in plants, such as whole grains, legumes, vegetables, fruits, seeds, and nuts (Table 4-2). Sources of dietary fiber usually contain other macronutrients, such as digestible carbohydrate and protein normally found in foods. During food processing, many compounds are added that have the same physiological effect as naturally occurring fiber, but the food may not have other health benefits, such as vitamins and minerals or alter satiety.
Table 4-2
| Physiological Response | ||||
| Type of Fiber | Dietary Fiber Sources | Laxation | Normalization of Blood Lipid Concentration | Attenuation of Blood Glucose Response |
| Cellulose | Whole-wheat, whole rye, bran, cabbage family, peas/beans, apples, root vegetables, fresh tomatoes | Yes | Neutral | Neutral |
| Gums and mucilages | Oats, dried beans, legumes, brown rice, barley, guar | Neutral | Yes | Yes |
| Hemicellulose | Bran, cereals, whole grains, dried beans | Yes | Unknown | Unknown |
| Lignin (noncarbohydrate)* | Fruits and edible seeds, mature vegetables, whole grains, flax seed | Yes | Unknown | Unknown |
| Pectin | Apples, citrus fruits, berries, carrots | Somewhat | Yes | Yes |
| Psyllium | Psyllium seeds, high-fiber cereals | Yes | Yes | Yes |
*Also classified as a phytochemical.
Data from Institute of Medicine of the National Academies: Dietary reference intakes: energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids, Washington, DC, 2002, National Academies Press.
Total fiber is the sum of dietary fiber and functional (added) fiber. Many fibers can be classified either as dietary fiber or functional fiber, depending on whether they are a natural component of the food or added to the food during processing. Plant-based foods are a good source of dietary fiber, but commercially developed functional fibers for use in processed foods also have a beneficial role in health. Various types of fibers have distinct properties resulting in different physiological effects (see Table 4-2).
Physiological Roles
Energy
The principal role of absorbed sugars is to provide a source of energy for body functions and activity and for heat to maintain body temperature. Glucose is the preferred source of energy for the brain and central nervous system, red blood cells, and lens of the eye. When carbohydrate intake is restricted, fat and protein stores may be used as an energy source. Although many organs can use fats for energy, glucose is the preferred fuel. Carbohydrate, whether it was originally from a sugar or a starch, provides 4 kcal/g. Because of incomplete absorption, sugar alcohols contribute varying amounts of kilocalories (see Table 4-1). Glycogen stores are a readily available source of glucose for the tissues.
Normal Fat Metabolism
Oxidation of fats requires the presence of some carbohydrates. When carbohydrate intake is low, the body relies on energy from fat intake or stores. As detailed in Chapter 2, when fats are metabolized faster than the body can oxidize them, intermediate products, called ketone bodies, may accumulate. Ketones are normal products of lipid metabolism in the liver; muscles can use ketones for energy only if adequate amounts of glucose are available. An accumulation of ketones in the blood, or incompletely oxidized fatty products, results in ketosis.
Gastrointestinal Motility
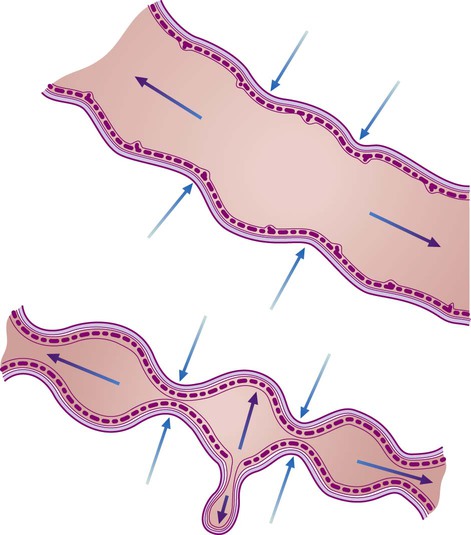
Dietary and certain functional fibers, particularly those that are poorly fermented, improve fecal bulk and laxation, ameliorate constipation, and perform various other functions (Table 4-2). Dietary fiber and functional fibers accelerate transit rate (the time it takes for waste products to move through the intestine) in individuals with a slow transit time (constipation). Viscous fiber decreases transit rate in individuals with a rapid transit time (diarrhea). The ability of fiber to bind water in the intestine and increase bulk from nondigestible substances decreases the length of time waste products are in the alimentary tract. An increased transit time lengthens the duration of tissue exposure to cancer-causing nitrogenous waste products. An added benefit of fiber is its stool-softening ability, which helps prevent constipation. Fiber in the colon increases stool bulk, exercising digestive tract muscles by increasing the radius of the colon and preventing the muscle from being chronically contracted. As muscle tone is maintained and colonic pressure declines, the gut is able to resist bulging out into pouches known as diverticula (Fig. 4-3).
Fiber-rich foods are not energy-dense and are retained longer in the stomach. They may cause one to feel full on a fewer number of kilocalories. Whether fiber plays a significant role in weight management has yet to be determined. Table 4-3 provides guidelines for assisting patients in increasing dietary fiber.
Table 4-3
Guidelines for developing a high-fiber diet
| Principles | Guidelines |
| Before recommending any changes, evaluate the patient’s fiber and fluid intake. For patients ≤50 years old, the optimal level of dietary fiber is 38 g for men and 25 g for women; for patients ≥51 years old, the optimal level of dietary fiber is 30 g for men and 21 g for women | Fiber normalizes bowel movements to once or twice a day by either speeding or slowing the transit rate of food through the gastrointestinal tract. Food-preservation methods, such as cooking and freezing, only slightly decrease fiber content; however, grinding or pureeing foods may have pronounced effects on fiber action. |
| Rather than fiber supplements, foods that contain soluble and insoluble fibers are the best way to increase fiber | Include two to four servings daily of fruits, especially those with skins (e.g., figs, pears, apricots, nectarines, raisins, blueberries) and edible seeds (e.g., blackberries, raspberries, strawberries). Include three to five servings of vegetables daily, especially sweet potatoes, carrots, mushrooms, raw onions, pumpkin, spinach, turnip greens, kale, Brussels sprouts, parsnips, English peas, beets, okra, and broccoli. Vegetables (e.g., mushrooms, peppers, onions, tomatoes) can be added to meatloaf, spaghetti, chili, omelets, or scrambled eggs. Serve raw vegetables with low-fat dip as appetizers or snacks. (Take advantage of ready-to-use vegetables.) Add leafy greens, tomatoes, and sprouts to sandwiches. Include raw vegetables (e.g., zucchini, carrots, celery sticks) in brown-bag lunches. Choose fresh fruits and vegetables or plain popcorn instead of fried chips and cookies. Dietary fiber comes principally from whole-grain products; brown color is no guarantee of whole-grain content. Look for breads and cereals that list “whole grain” or “whole wheat” first in the ingredients list. Choose cereals with at least 2 g of fiber (5 g is ideal), but no more than 2 g of fat per serving. Experiment with brown rice, barley, whole-wheat pasta, and bulgur. Supplements made with concentrated or purified dietary fiber lack the nutritional balance provided by a varied diet that contains fruits, vegetables, whole-grain products, and legumes. Large amounts of purified fiber such as lignin and bran may result in important minerals, especially calcium, iron, and zinc, being bound by the fiber and excreted. |
| Fiber absorbs water in the intestines, so adequate fluids are important to keep the intestinal contents moving | Ensure intake of 10-12 cups of decaffeinated fluids a day to avoid problems such as fecal impactions. |
| Increase high-fiber foods gradually. Begin with 5- to 10-g increments to avoid adverse side effects. At least 6-8 weeks should be allowed for adaptation to prevent flatulence, abdominal cramping, and diarrhea/constipation | Substitute whole-wheat flour for one-quarter or one-half of the white flour in baked goods. Add bran, bran flakes, wheat germ, chopped nuts, seeds, or oatmeal to mixed meat dishes, casseroles, salads, cooked cereal, cookies, breads, muffins, and pancake batter. Use whole-grain crackers and unbuttered popcorn. Incorporate beans into soups, casseroles, nachos, or a salad. Use bran flakes for a crispy coating on meats or fish. |
Stay updated, free dental videos. Join our Telegram channelVIDEdental - Online dental courses
 Get VIDEdental app for watching clinical videos
Get VIDEdental app for watching clinical videos

|