Candidosis (candidiasis)




INTRODUCTION
Some 50% of the normal population harbour (carry) the fungus Candida albicans as a normal oral commensal mainly on the posterior dorsum of tongue (without any disease) and are therefore termed ‘Candida carriers’. The opportunistic pathogen grows either as yeasts or hyphae (i.e. it is a dimorphic fungus). Actual infection with Candida (usually Candida albicans) is common mainly in people who are otherwise unwell; candidosis is thus called a ‘disease of the diseased’. The importance of Candida has increased greatly, particularly as the HIV pandemic extends since, when host defences are compromised, Candida typically colonizes mucocutaneous surfaces and causes only superficial infections but in immunocompromised people candidosis is commonly oro-pharyngeal and can be a portal for entry into deeper tissues and invasive candidosis (see Chs 53 and 54).
AETIOLOGY
Host defences against Candida species include the following:
 Oral epithelium: a physical barrier.
Oral epithelium: a physical barrier.
 Microbial interactions: competition and inhibition by the oral flora.
Microbial interactions: competition and inhibition by the oral flora.

 lysozyme (muramidase): can damage Candida, stimulate phagocytosis and agglutinate Candida
lysozyme (muramidase): can damage Candida, stimulate phagocytosis and agglutinate Candida

 lactoperoxidase: is anticandidal via multiple factors (H2O2 and halides)
lactoperoxidase: is anticandidal via multiple factors (H2O2 and halides)
 glycoproteins antigenically similar to blood group antigens – affect adherence to mucosa
glycoproteins antigenically similar to blood group antigens – affect adherence to mucosa





 Oral immune defences, which include mainly cell-mediated responses:
Oral immune defences, which include mainly cell-mediated responses:
 T cells and phagocytes. The full expression of phagocyte effectiveness is dependent on augmentation by cytokines synthesized or induced by T cells, such as lymphokines and IFN-γ. Polymorphonuclear leukocytes (PMNL) and macrophages phagocytose and produce cytokines, such as: myeloperoxidase, tumour necrosis factor (TNF), interferon-γ (IFN-γ), nitric oxide and granulocyte-macrophage colony stimulating factor (GM-CSF).
T cells and phagocytes. The full expression of phagocyte effectiveness is dependent on augmentation by cytokines synthesized or induced by T cells, such as lymphokines and IFN-γ. Polymorphonuclear leukocytes (PMNL) and macrophages phagocytose and produce cytokines, such as: myeloperoxidase, tumour necrosis factor (TNF), interferon-γ (IFN-γ), nitric oxide and granulocyte-macrophage colony stimulating factor (GM-CSF).
 Salivary sIgA antibodies: which aggregate Candida organisms and/or prevent adherence.
Salivary sIgA antibodies: which aggregate Candida organisms and/or prevent adherence.
PATHOGENESIS
 C. albicans can switch frequently and reversibly between several variant, heritable, phenotypes associated with changes in micromorphology, physiology and virulence (‘colony switching’).
C. albicans can switch frequently and reversibly between several variant, heritable, phenotypes associated with changes in micromorphology, physiology and virulence (‘colony switching’).


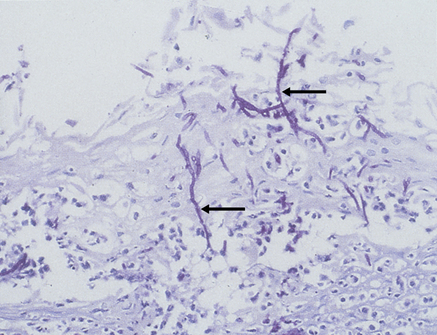
 Hyphae invade the superficial epithelium and penetrate, via enzymes such as the phospholipases, lysophospholipases and aspartyl proteinase (secretory aspartyl proteinases; SAP) (Fig. 39.1) as far as the stratum spinosum.
Hyphae invade the superficial epithelium and penetrate, via enzymes such as the phospholipases, lysophospholipases and aspartyl proteinase (secretory aspartyl proteinases; SAP) (Fig. 39.1) as far as the stratum spinosum.













CLINICAL FEATURES
Candidosis (candidiasis; moniliasis) is the state when Candida species cause lesions or symptoms:
 The most dominant oral Candida species, in decreasing order of frequency, are:
The most dominant oral Candida species, in decreasing order of frequency, are:









 Antifungal resistance is an increasingly serious clinical reality.
Antifungal resistance is an increasingly serious clinical reality.
Symptomatic oral candidosis presents as mainly:
 white lesions, in which hyphal forms are common: these include thrush, candidal leukoplakia and chronic mucocutaneous candidosis
white lesions, in which hyphal forms are common: these include thrush, candidal leukoplakia and chronic mucocutaneous candidosis

Factors that can increase the liability to oral candidosis are shown in Box 39.1. Candidosis may also affect or spread from or to the mouth, from:
BOX 39.1 Factors predisposing to oral candidosis
Local factors influencing oral immunity or ecology, including:











 pharynx, oesophagus, and rarely lungs, liver or elsewhere
pharynx, oesophagus, and rarely lungs, liver or elsewhere
 anogenital region: candidosis can also be sexually shared (e.g. by vaginal, oral or anal sex)
anogenital region: candidosis can also be sexually shared (e.g. by vaginal, oral or anal sex)

By tradition, the most frequently adopted classification of oral candidosis has been into (Box 39.2):
BOX 39.2 Classification of oral candidosis














DIAGNOSIS OF CANDIDOSIS
Diagnosis can, if necessary, be supported by:
 identification of blastospores and pseudohyphae in stained smears from a lesion
identification of blastospores and pseudohyphae in stained smears from a lesion
 culture, usually on Sabouraud or dextrose Sabouraud medium
culture, usually on Sabouraud or dextrose Sabouraud medium
 PCR studies – mainly for detection of invasive candidosis
PCR studies – mainly for detection of invasive candidosis
 occasionally by histology stained by periodic acid–Schiff (PAS).
occasionally by histology stained by periodic acid–Schiff (PAS).


Tests of immune function are indicated mainly in HIV disease or chronic mucocutaneous candidosis.
Since some endocrine disorders may be associated with chronic mucocutaneous candidosis, tests of thyroid, parathyroid and adrenocortical function are warranted in selected individuals (Table 39.1).
Table 39.1
Aids that might be helpful in diagnosis/prognosis/management in some patients suspected of having candidosis (candidiasis)*
| In most cases | In some cases |
| Culture and sensitivity Full blood picture |
Biopsy Serum ferritin, vitamin B12 and corrected whole blood folate levels ESR CD4 counts Serology for antiacetylcholine receptor antibodies Plasma cortisol Plasma calcium and phosphate levels |
TREATMENT OF CANDIDOSIS (see also Chs 4 and 5)
Few patients have spontaneous remission unless the condition is solely related to, for example, the use of an antimicrobial, or a topical corticosteroid, and thus, in other cases, treatment is often indicated (Table 39.2). Often, in the treatment of fungal infections, attention to the underlying cause will avoid the need for prolonged or repeated courses of treatment. Intermittent or prolonged topical antifungal treatment may be necessary where the underlying cause is unavoidable or incurable. Treatment includes the following measures:
Table 39.2
Regimens that might be helpful in management of patient suspected of having candidosis
| Regimen | Use in primary or secondary care |
| Beneficial | Nystatin Miconazole Fluconazole Itraconazole |
| Unproven effectiveness | Chlorhexidine Ciclopirox Genti/> |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


