Intraoral Radiographic Anatomical Landmarks
The landmarks discussed here are those that are seen in intraoral periapical radiographs.
Landmarks Common to Both the Maxillary and Mandibular Radiographs
 Teeth—enamel cap, dentin, cementum, pulp
Teeth—enamel cap, dentin, cementum, pulp

 Alveolar bone—lamina dura, alveolar crestal bone, marrow spaces and trabecular bone.
Alveolar bone—lamina dura, alveolar crestal bone, marrow spaces and trabecular bone.
Teeth
Enamel cap, dentin, cementum, pulp.
Enamel appears almost snow white and is seen extending from the neck of the tooth, i.e. the cementoenamel junction from one side to the other covering the tooth like a cap (enamel cap). It is the most mineralized structure on the radiograph (90% mineralized) and appears more radiopaque than other structures (Figure 1).
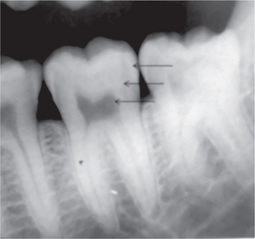
Figure 1 Radiograph showing enamel, dentin and pulp. Enamel is the most radiopaque and pulp is radiolucent
Cementum is not appreciated radiographically because the contrast between it and dentin is minimal. Cementum is 50% mineralized.
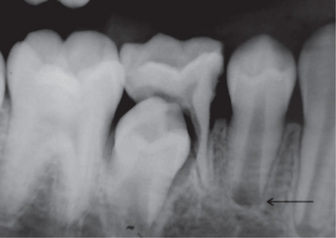
In a developing tooth, the pulp canal diverges and the walls of the root taper to a knife edge. A small round area of radiolucency is seen at the root tip which is surrounded by a thin layer of hyperostotic bone which is the dental papilla enclosed by the bony crypt (Figure 2).
Periodontal Ligament Space
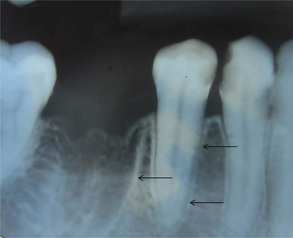
The periodontal ligament space is seen as a radiolucent area between the root surface and the lamina dura. It is seen all around the root extending from the alveolar crest on one side to the other (Figure 3). The width of the periodontal ligament space varies from 0.15 to 0.36 mm; it is generally thinner in the middle third of the root and wider near the alveolar crest and the apical region of the root. However due to projection errors, the periodontal ligament space may not be discernible on some radiographs.

Alveolar Bone
Lamina dura, alveolar crestal bone, cancellous trabecular bone.
Lamina dura
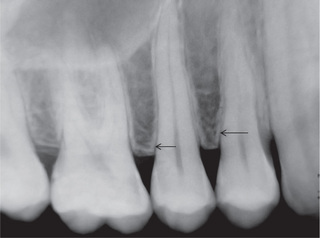
Lamina dura is a radiographic term used to describe alveolar bone proper (cortical bone), which forms the sockets of teeth. It is also considered to be a ‘specialized’ continuation of the cortical plate. Radiographically, lamina dura is seen as a well-defined radiopaque line that surrounds the roots of teeth in health (Figure 4). The appearance of lamina dura on a radiograph is because of the attenuation of the X-ray beam as it passes through the thin layer of bone tangentially.
Alveolar crest
Crest of the alveolar bone is a radiopaque structure. It is seen as a continuation of the lamina dura (cortical bone). The junction between the alveolar crest and lamina dura is seen as a sharp well-defined angle. Generally the crest of the alveolar ridge is 1.5 mm apical to the cementoenamel junction. In the anterior teeth, the alveolar crest terminates as a pointed projection and in the posterior teeth it appears flat and parallel to the cementoenamel junction (Figures 5 and 6).

Cancellous bone
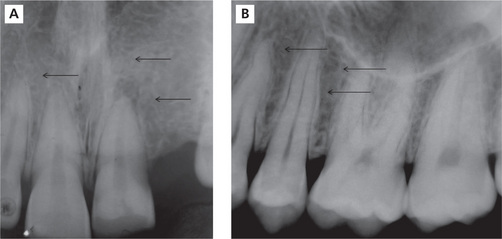
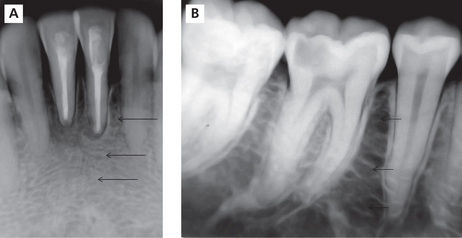
In the maxillary anterior region, the trabeculae are fine and dense and in the posterior region the bone marrow spaces are relatively larger and oriented irregularly (Figure 7A). In the anterior region of the mandible, the trabeculae are fewer in number and oriented horizontally. In the posterior region of the mandible the bone marrow spaces are larger (Figure 7B).
Landmarks Unique to the Maxillary Intraoral Periapical Radiograph


 Nasal fossae and floor of the nasal fossae
Nasal fossae and floor of the nasal fossae






 Superior foramina of the nasopalatine canal
Superior foramina of the nasopalatine canal









Intermaxillary suture/median suture
Nasal fossae and floor of the nasal fossa
Radiographic appearance (Figure 9)
The floor of the nasal fossae appear as well-defined radiopaque lines that extend bilaterally on either side of the anterior nasal spine. The radiolucent region above the floor of the nasal fossae is the inferior portion of the nasal fossa.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


