Chapter 3
Impression Procedures for Complete Dentures
Aim
The aim of this chapter is to discuss the theory for achieving complete denture retention and the importance of impression procedures.
Outcome
At the end of this chapter, the clinician should understand that creating a retentive denture is reliant on a good understanding of the anatomy of the denture-bearing area, and physical and physiological factors. Recording an impression is a process which requires consideration of the action of the sulcus, the condition of the denture-bearing area, the quality and quantity of saliva and finally the materials used to record the impressions. It must be seen as a two-stage process, with the primary and secondary impression stages having distinct, important functions. If sufficient attention is paid to recording good quality primary and secondary impressions, then the denture should be retentive.
Impression Theory
Retentive complete dentures are reliant on the interplay between forces of retention, stability and support. To describe these succinctly, retention depends on forces which resist displacement of the denture away from the denture-bearing area; stability relies on resisting forces likely to displace the denture laterally or anteroposteriorly; and support is provided by factors which resist displacement of the denture into the denture-bearing tissues. The important relationship between these forces is shown in Fig 3-1. Although this chapter is devoted to a discussion of impression making, the reader should bear in mind that these factors are inter-related. If, for example, one has created a retentive denture but introduced occlusal errors into the occlusal scheme of the dentures, then the resultant instability of the dentures caused by the unbalanced occlusion may overcome the forces designed to retain the denture. Similarly, apparently satisfactory retentive forces can be overcome by an unstable denture-bearing area such as a flabby alveolar ridge.
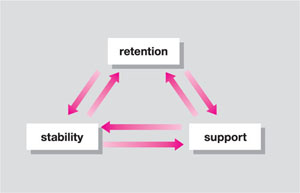
Fig 3-1 Relationship between retention, stability and support. The retention of complete dentures is dependent on the interaction between these forces.
Forces which will make a complete denture retentive have been described as (a) physiological forces and, (b) physical forces.
-
Physiological forces – These forces are applied to the polished surfaces of the dentures by the muscles of the lips, the cheeks and the tongue. They rely on the patient’s ability to learn a complex series of neuromuscular reflexes, and this varies from patient to patient. The patient has to learn to use these muscles to exert retentive forces on the polished surfaces of the dentures during functional movements. Fish described how the clinician should shape the polished surfaces of the dentures to enhance these physiological forces of retention (Fig 3-2). These forces of retention can be harnessed to overcome some of the limitations of complete dentures, and may help explain why patients can control technically inadequate dentures. It is possible that the ability of patients to control dentures diminishes with age, and keeping a familiar polished surface shape may be critical to the outcome of new replacement complete dentures. This is the theoretical basis for the copy denture technique described in Chapter 9.
-
Physical forces – Forces of adhesion, cohesion and surface tension can be harnessed to improve denture retention. In clinical terms, this involves creating a peripheral seal. Air must be excluded between the fitting surface of the denture and the denture-bearing tissues, and an intact salivary film allowed to form on the impression surface of the denture. If this is achieved, forces of cohesion will act to keep the salivary film intact, whilst forces of adhesion and surface tension will act to attract saliva to the denture and the denture-bearing tissues. These forces will be harnessed only if the denture is placed on compressible tissues, and it is therefore important that the clinician identifies these in the mouth. The elastic nature of these tissues allows them to recoil around the periphery of the denture when compressed. The compressible areas of soft tissue in the denture-bearing area are the sulci, the attached part of the soft palate and the retromolar pads in the mandible. If the denture is not placed over these areas, then air will escape into the area above the fitting surface and disrupt the layer of saliva. Further factors which influence the physical forces of retention are:
-
surface area – the greater the area of coverage, the more retentive the denture will be
-
the quantity of saliva – retention decreases as salivary flow diminishes
-
the quality of saliva – if saliva is thick with a high mucus content, the dentures are unlikely to be retentive
-
the space between the fitting surface of the denture and the denture-bearing area should be as thin as possible.
-
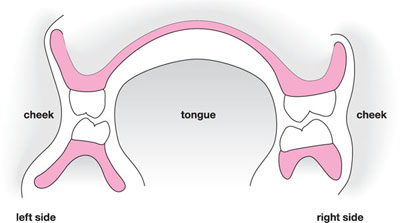
Fig 3-2 Action of muscles on polished surfaces of complete dentures.
Anatomy of the Denture-bearing Area:
Two aspects should be considered: (a) gross anatomy of the maxillary and mandibular denture-bearing area; and (b) the histology of the denture-bearing tissues. The retention of complete replacement dentures is influenced by the activity of muscles which define the buccal, labial and lingual sulci, frenal attachments, and the soft palate. These will influence the shape of the periphery of the dentures. Muscle groups also influence the shape of the polished surfaces of the dentures. The muscle groups involved are listed in Table 3-1.
| Maxilla | Mandible |
| Periphery | Periphery (buccal) |
| buccinator | buccinator |
| levator anguli oris | depressor labii inferioris |
| incisivus superioris | mentalis |
| buccal frena | |
| labial frena | Periphery (lingual) |
| muscles of the soft palate | superior constrictor |
| pterygomandibular raphe | |
| palatoglossus | |
| mylohyoid | |
| genioglossus | |
| lingual frenum | |
| Polished surface shape | Polished surface shape |
| modiolus | anterior border of masseter |
| tongue | |
| modiolus |
The anatomy of the denture-bearing area in the maxilla is further defined by:
-
the residual alveolar ridge
-
the root of the zygoma
-
the hamular notch
-
the maxillary tuberosities
-
the attached part of the soft palate.
and in the mandible by:
-
the residual alveolar ridge
-
the external oblique ridge
-
the retromolar pads.
The oral mucosa consists of epithelium and connective tissue. It covers the palate and the alveolar ridges, and extends over the muscles of the palate, cheeks and floor of the mouth. In areas where there is friction, the epithelium has the potential to produce keratin which increases resistance to trauma. In certain areas of the mouth, such as the sulci, the oral mucosa is separated from the underlying muscle by a layer of submucosa. This tissue is compressible and suitable for loading with a denture. Areas where the oral mucosa is tightly bound to bone, such as the hard palate, do not have a layer of submucosa and are not compressible. When severe alveolar resorption occurs, prominent spicules of bone such as the genial tubercles can become superficial. The oral mucosa is tightly bound to this bone and offers poor support for a complete denture. These areas should be relieved by placing tin foil on the master cast prior to processing the denture base.
Primary Impressions
The aim of the primary impression is to record the entire denture-bearing area. Failure to record the denture-bearing area on the primary impression will create difficulties in recording a satisfactory definitive impression and ultimately result in a poorly retentive denture. Consequently, it is unwise to disregard the importance of having a satisfactory primary impression in the hope that deficiencies will be rectified in the definitive impression. The nature of primary impressions is such that control of the tissues when recording the impression is minimal, and thus the impression will be overextended. If a denture is made on a model cast from such an impression, then it too will be overextended and not retentive.
Primary impressions should be recorded in rigid stock trays. Examples of edentulous stock trays are shown in Fig 3-3. When recording a primary impression, the clinician should select a tray that most closely fits the denture-bearing area. If the tray is grossly underextended, then green stick tracing compound or beading wax can be added to the tray to improve extension. If the denture-bearing area is particularly small, then overextension of the tray may be a probl/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


