Esthetics in Tooth Display and Smile Design
Bjørn U. Zachrisson
The orthodontic profession has always been in pursuit of the ideal dentition. At present, we are on the threshold of a paradigm shift that apparently will change the fundamental conceptual basis of orthodontics and the traditional emphasis in diagnosis and treatment planning.1,2 The former emphasis on dental and skeletal components is still valid but greater attention than before is now required to the soft tissue aspects of orthodontics. In an effort to create natural esthetics, the orthodontist must give careful consideration to the patient in his or her entirety. Individual attributes of a tooth or segment of teeth may represent only part of the story, because teeth do not exist individually and separate from the patient to whom they belong. Combinations of tooth positions can create an effect that is greater than, equal to, or less than the sum of the parts.3 The discipline of esthetics in orthodontics can be broken down into at least four parts: microesthetics (the elements that make teeth look like teeth), gingival esthetics, macroesthetics (the principles that apply when groupings of individual teeth are considered), and facial esthetics.3 This chapter will focus on the principles of macroesthetics and facial esthetics in orthodontics and how to apply them clinically. The dynamic relationship between the teeth and the surrounding soft tissues during and after orthodontic corrections and the patient’s facial characteristics will be emphasized. The display (amount and shape of crown structure that shows in various views and lip positions) will be related to age, sex, and facial characteristics. The purpose is to provide guidelines for orthodontists on how to analyze esthetic factors by viewing the patient from the front and to discuss some new concepts on how to achieve the desirable characteristics of tooth display in the vertical and transverse dimensions during normal social interaction.
Evaluating Esthetics in the Dentist’s Chair
Esthetics, which is derived from the Greek word for “perception,” deals with beauty and the beautiful. It may be divided into two dimensions: objective (admirable) and subjective (enjoyable) beauty.4 Objective beauty implies that the object possesses properties that make it unmistakably praiseworthy. Subjective beauty is value-laden and is related to the tastes of the person contemplating it. Contemporary techniques in orthodontics should lend objective esthetics to the entire orofacial complex, involving unity, form, structure, balance, color, function, and display of the dentition. In addition, the creation of subjective beauty according to an individual orthodontist’s preferences may enhance the cosmetic value of the treatment rendered to each patient.
In discussing the principles of visual perception and its clinical application to dentofacial esthetics, Lombardi5 remarked that detailed esthetic judgments can be made only by viewing patients from the front, in conversation, and observing facial expressions and smiling. The traditional dentist’s view from above and behind the patient is skewed, differing markedly from the “true” perception of the patient in a mirror or by other persons during normal social interaction. For example, it is not possible to gain adequate information on such details as midline alignment (maxillary and mandibular relative to facial) and right-left symmetry of canine and premolar crown torque (Fig. 3-1, A) unless the patient is observed directly from the front (Fig. 3-1, B). A direct “eye-to-eye” view of the dentition can, in fact, be obtained when the patient is sitting in the dental chair6; the trick is to move the patient’s head to the side of the headrest (see Fig. 3-1, B). With this method it is possible to analyze important esthetic factors during the treatment (Fig. 3-1, C and D), such as:
• Crown lengths of the upper and lower incisors
• Incisal edge contours (before and after recontouring)
• Position and symmetry of gingival margin levels on the upper and lower anterior teeth
• Axial inclinations of all anterior teeth
• Midlines (maxillary to mandibular and facial)
• Connector areas (the zone in which two adjacent teeth appear to touch)
• Symmetry and degree of crown torque of the canines and premolars
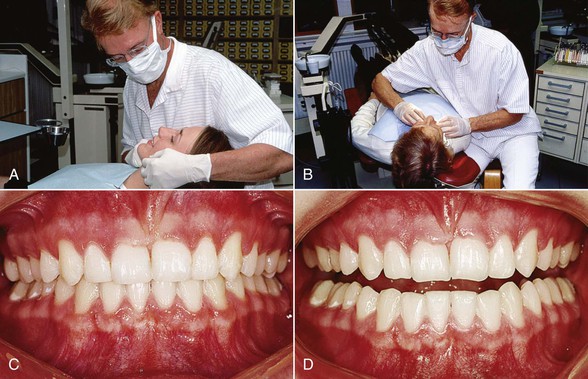
Figure 3-1 A, Unsuitable position for evaluating esthetics during treatment. Moving the patient’s head to the side of the headrest (B) allows direct frontal view of dentition (C) and a realistic impression of esthetic features. D, The incisal edge contours can be examined on slight mouth opening.
It is important for a successful outcome that the clinician has learned to look at all of these aspects and has the ability to make the necessary corrections while the fixed appliances are still on, because “you can only change what you see.”7 After carefully studying the patient’s dentition, the orthodontist can make the required finishing archwire bends and perform any other esthetic procedures needed. For analysis of tooth display when speaking and smiling and viewing the buccal corridors on smiling, a better impression is obtained when the patient is sitting up or standing in front of the dentist.5,6
Standards of Normality
It is useful for esthetic oral rehabilitations to describe some average desirable characteristic features of smiles. These normative standards may serve as a guideline for enhancement of esthetics for the anterior component of the dentition.
Smile Type: Incisor and Gingival Display
Lip coverage of the maxillary incisors in full smiles is generally distinguished into three types: low, average, and high smiles.8 The most frequent type8,9 (found in about 70% of the young adult population) is the average smile that reveals 75% to 100% of the upper incisors. The low smile displays less than 75% of the maxillary incisors in a full smile and is found in about 20% of the population, whereas the high smile reveals the complete cervicoincisal length of the upper incisors and a contiguous band of gingiva and occurs in about 10% of the U.S. population.8 A fourth type of lip line height may be defined as a “gummy” smile, which occurs when patients show more than 4-mm of gingiva on smiling (discussed later in the chapter).10,11
Upper lip coverage will always increase with age and therefore the percentage of high smiles may be greater among younger age groups12,13 and smaller among older adults.9,14 There is also a sexual dimorphism in that low smile lines are predominantly a male characteristic and high smiles are predominantly a female characteristic.8
It is noteworthy that some marginal gingival display in smiling is not as objectionable to laypersons as orthodontists may imagine.10,13 We should therefore look on a moderately high smile type as an acceptable anatomic variation well within the usual range of lip-tooth-jaw relationships, especially among women.12,13
Smile Arc15,16 (Smile Curve)
The relationship of the maxillary incisal curve to the inner contour of the lower lip can be divided into three types: parallel, straight, and reverse. In a survey of young adults in the Los Angeles area, Tjan et al.8 found that a great majority (85%) had a maxillary incisal smile curve parallel to the inner contour of the lower lip, 14% showed a straight rather than a curved line, and only 1% had a reverse smile curve. Since parallelism is the normal finding in untreated persons, it is an optimal goal for objective beauty in esthetic oral rehabilitations,17,18 including orthodontic (Figs. 3-2 and 3-3) and orthodontic-prosthetic treatments (Fig. 3-4). A straight or reverse smile curve may contribute to a less attractive facial appearance.5,17 The reverse curve is frequently associated with marked abrasive wear of the upper incisors.

Figure 3-2 A and B, Esthetic smile curve (arc) with parallelism between maxillary teeth and inner contour of lower lip in four-premolar extraction case. Upright canine and premolar crowns contribute to fullness of smile.

Figure 3-3 A–D, Improvement in parallelism between maxillary anterior tooth curve and lower lip contour with orthodontic treatment in adult female bimaxillary crowding case. Cant of maxillary central incisor midline is corrected.

Figure 3-4 A–D, Orthodontic-prosthetic interdisciplinary approach to improve parallelism between maxillary incisor curve and lower lip contour in adult female Class II, Division 2 malocclusion with worn central incisors. Four porcelain laminate veneers (courtesy Dr. S. Toreskog, Göteborg, Sweden) were used to restore and elongate the maxillary incisors.
Number of Teeth Displayed in the Smile
The California survey8 also revealed that in a typical or average smile in young adults, the six maxillary anterior teeth and the first or second premolars are displayed. The number of teeth displayed in the full smiles of 454 students was six anteriors only, 7%; six anteriors and first premolars, 48.5%; six anteriors and first and second premolars, 40.5%; and six anteriors, first and second premolars, and first molars, 4%.
Vertical Position of the Incisors
Normal Age Changes in Lip-Incisor Relationship
Progressive changes with age on upper and lower lip positions are caused by the effects of gravity. Some normative studies on the optimal vertical incisor positions in the faces of persons in different age groups are available. Peck et al.13 showed that the normal display of maxillary incisors with relaxed lips at 15 years of age was 4.7-mm (standard deviation [SD] 2.0-mm) for boys and 5.3-mm (SD 1.8-mm) for girls. The sexual dimorphism is evident at all ages. For adults, Vig and Brundo14 have provided normative mean values for different age groups (Table 3-1). Dong et al.19 compared the age changes in maxillary and mandibular incisor display at rest and when smiling (Fig. 3-5) and confirmed the observations that the age changes with relaxed lips were dramatic (Fig. 3-6). Mandibular incisor display shows a corresponding increase with age. The amount of mandibular incisor display after age 60 is approximately equal to the amount of maxillary incisor display before age 30 (see Fig. 3-5 and Fig. 3-6, D).
TABLE 3-1
Maxillary and Mandibular Incisor Display with Lips Gently Parted (in mm)
| Age Group (Years) | Maxillary Central Incisor | Mandibular Central Incisor |
| Up to 30 | 3.5 | 0.5 |
| 30–40 | 1.5 | 1.0 |
| 40–50 | 1.0 | 2.0 |
| 50–60 | 0.5 | 2.5 |
| Over 60 | 0.0 | 3.0 |
Modified from Vig RG, Brundo GC. The kinetics of anterior tooth display. J Prosthet Dent. 1978;39:502–504.
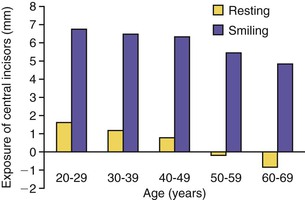
Figure 3-5 Comparison of maxillary incisor display by age with lips at rest and on smiling. (Reproduced with permission from Dong JK, Cho HW, Oh SC. The esthetics of the smile: a review of some recent studies. Int J Prosthodont. 1999;12:9–19.)

Figure 3-6 Age changes in vertical incisor display with relaxed lips, demonstrated by female patients aged 25 years (A and C) and 65 years (B and D). Note that the younger woman shows only maxillary incisors, whereas the older woman shows only mandibular incisors.
There is a close correlation between the incisor exposure at rest and during normal speech.20,21 The tooth display in speaking may be every bit as important as the tooth display in smiling to express personality and age. The most important information related to esthetics in treatment planning is obtained when the patient is observed during normal conversation. The tooth display on smiling will not provide the same information since when a person is smiling, the upper lip is raised actively by three different muscle groups.22 For this reason, nearly everyone, irrespective of age, will display the maxillary incisors nicely in the full smile, even if only the mandibular incisors are visible during their speech. In other words, the age changes in incisor display are much more pronounced and apparent with the lips relaxed and when the patient is speaking than when he or she is smiling (Fig. 3-7).15
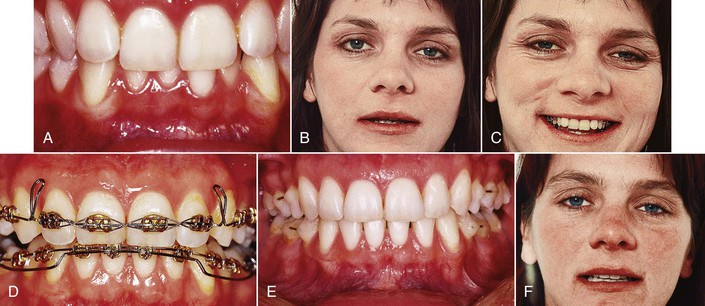
Figure 3-7 Deep anterior overbite in a 30-year-old female patient before (A–C), during (D), and after (E and F) orthodontic treatment. The initial maxillary incisor display with lips at rest (B) corresponds to a much older person. For this reason, the maxillary central incisors were extruded with step-down bends in the archwire and the mandibular incisors were intruded using an overlay base arch (D). Final result shows overbite correction (E) and a maxillary incisor display more relevant to the patient’s age (F).
The sagging of the perioral soft tissue is partly due to the natural flattening, stretching, and decreasing elasticity of the skin.23 The upper lip becomes longer and hides more and more of the maxillary incisors, while the drooping of the lower lip gradually exposes more of the mandibular incisors. As a consequence, show of maxillary incisors with relaxed lips signifies youth and beauty, whereas display of mandibular incisors is a characteristic of the elderly (see Fig. 3-6). The importance of the vertical dimension in tooth display has been demonstrated in prosthetic dentistry13,14 and in orthognathic surgery involving maxillary repositioning.24,25
The guide for tooth position planning in orthodontic treatment should start with an appraisal of the position of the maxillary central incisal edge relative to the upper lip.26,27
This assessment is made with the patient’s upper lip at rest, using a millimeter ruler or periodontal probe. This incisor position can be either acceptable or unacceptable, depending on the patient’s age. The clinical guideline should be that the maxillary incisors should be moved in the vertical direction that improves their relationship to the resting lip position relative to the patient’s age (Figs. 3-8 and 3-9; see Fig. 3-7). The relaxed lip position is the most reproducible functional position. It can and should be used as the guide,26,27 whereas forced or posed smiles may vary considerably in the same patient and cannot be considered an accurate guide for incisor positioning.27
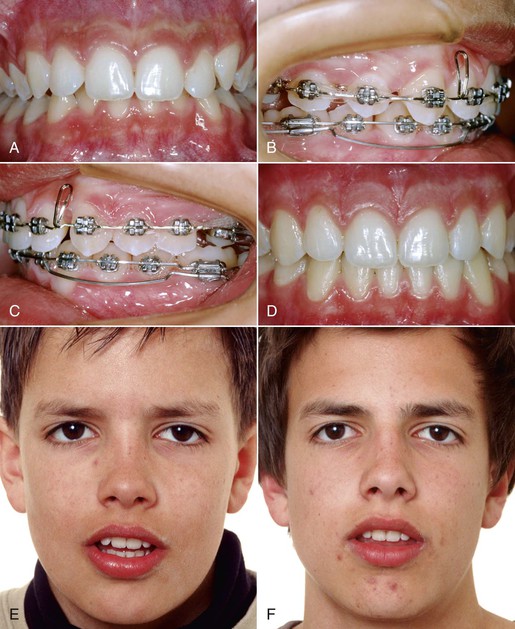
Figure 3-8 A and E, Young male patient with deep anterior overbite. E, Rest position photograph indicates that maxillary incisors should not be intruded. B and C, Mandibular incisor intrusion using 0.0175-inch × 0.025-inch CNA overlay arches from double tubes on the mandibular first molars. Final result demonstrates (D) overbite correction and (F) optimal maxillary incisor display with lips at rest.
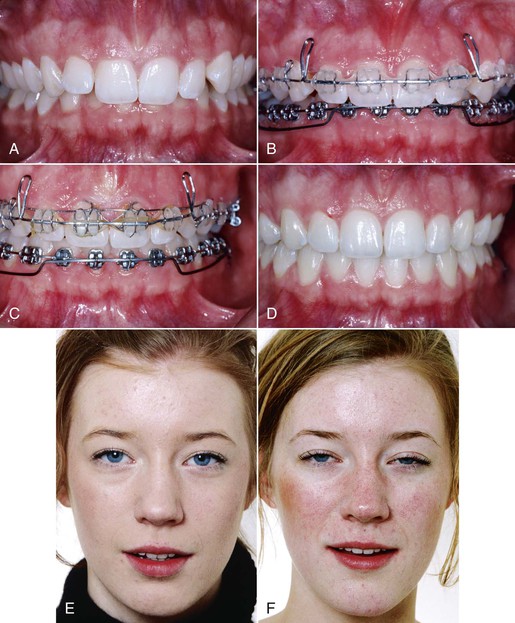
Figure 3-9 A and E, Eighteen-year-old female with Class II, Division 2 deep overbite malocclusion. E, The anterior overbite should not be treated with maxillary incisor intrusion, since the tooth display with lips at rest is good. B-D, The maxillary incisors were merely leveled and the deep bite correction was made with intrusion of the mandibular incisors. C, Von der Heydt torquing auxiliary was used to improve the maxillary incisor inclination. F, The incisor display with relaxed lips after treatment is unchanged.
Spontaneous smiling records may also be recommended for diagnostic purposes. Because of the dynamic nature of spontaneous smiling, dynamic video recording of the spontaneous smile should be preferred.9,20,21 Lip-tooth relationships follow a consistent pattern in natural rest position and during speech and spontaneous smiling.
Sex Differences
The sexual dimorphism in anterior tooth display implies that females have significantly more maxillary and less mandibular tooth exposure than males at all ages. In a group of adults, Vig and Brundo14 found almost twice as much maxillary anterior tooth display with the lips at rest in women (3.4-mm) as in men (1.9-mm). Men displayed much more of the mandibular incisors (1.2-mm compared to 0.5-mm).
Standardized Extraoral Records
A standardized procedure for recording the incisor display in (1) rest position (Fig. 3-10; see Figs. 3-4 to 3-9) and (2) a posed smile (see Figs. 3-2 to 3-4) both before and after orthodontic treatment is recommended and will help the clinician to avoid undesirable treatment effects on the maxillary incisor reveal. Each patient should be coached and asked to achieve the same lip position at least twice in succession before a photograph is taken. In rest position (instruct the patient to say “Emma” or “Mississippi”),6,28 the teeth should be slightly apart and both the perioral soft tissue and the mandibular posture must be unstrained. In the posed smile (instruct the patient to bite together, smile, and say “Cheee …”),6 the teeth should be lightly closed. As mentioned, the analysis of incisor display during spontaneous smiling should be made with video records.
Clinical Implications for Deep Overbite Correction
Average and Low Smile Types
The correction of deep anterior overbite can be made by various combinations of incisor intrusion and molar extrusion.29,30 The treatment concepts for deep overbite cases have changed significantly during the past 10 to 15 years. This is due to the increasing attention now being paid to the esthetic importance of the vertical display of the maxillary incisors during normal speech and with relaxed lips.6,7,26 While active intrusion of maxillary incisors with intrusion arches à la Burstone, utility arches à la Ricketts, overlay base-arches, and similar approaches has previously been considered a cornerstone of deep bite correction, the risk of too much intrusion (so-called “overintrusion”) with such approaches is apparent.28,30 Overintrusion may tend to hide the maxillary incisors behind the upper lip when the patient is speaking. Lindauer et al.30 compared the outcomes from two common procedures used to reduce deep overbite: maxillary incisor intrusion using an intrusion arch and posterior eruption using an anterior biteplate. Both the intrusion arch and the biteplate procedures effectively reduced overbite significantly over a relatively short period of treatment. The intrusion arch patients displayed significant reductions in maxillary incisor display (mean change from 5.4- to 3.0-mm) accompanying documented incisor intrusion. This means that a maxillary intrusion arch will lead to a premature aged oral appearance. Such a mistake can go undetected by the orthodontist unless the upper central incisors show on speaking and smiling is recorded and analyzed properly. With increasing age of the patient and concomitant drooping of the upper lip, an unesthetic incisor display at adolescence will predictably worsen with time.9,21
In a child or adolescent patient, maxillary incisor intrusion beyond 4- to 5-mm below the upper lip at rest represents overintrusion of these teeth and unwanted aging of the patient. In a young adult between 20 and 30 years of age, there should be at least 3-mm of maxillary incisors showing. For an adult 30 to 40 years of age, approximately 1.5-mm of the maxillary incisors should show at rest position of the lips, and at age 40 to 50 years, about 1-mm should show. In patients more than 50 to 60 years of age, the maxillary incisors normally should not show at all when the lips are relaxed (see Fig. 3-6). According to Frush and Fisher,31 an optimal incisor position for adults occurs when the maxillary lateral incisors show “when the patient is speaking seriously.” The tips of the lateral incisors should show in varying degrees according to the sex and age requirements.
The tooth-to-lip position at rest should be monitored constantly throughout the orthodontic treatment. Since no orthodontist would wish to make his or her patients look older than they really are, it is important to carefully analyze each patient’s tooth display on speaking before deciding whether maxillary intrusion mechanics should be used.28 In some deep overbite cases, extrusion rather than intrusion of the maxillary incisors may be indicated (see Fig. 3-7) or a combination of orthodontics and prosthetic crown lengthening with porcelain laminate veneers will be the method of choice (see Fig. 3-4).
From an esthetic point o/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


