Chapter 3
Crowning Root Canal Treated Teeth
Aim
To review the indications of crowning root-filled teeth, to describe the indications for different crown types and to provide clinical tips on the crowning of root canal treated teeth.
Outcome
At the end of this chapter, the reader should be able to decide whether or not a root canal treated tooth needs to be crowned and to choose the most appropriate type of crown.
Introduction
Decision-making in respect of the restoration of root canal treated teeth is a daily challenge in clinical practice. A variety of restorative approaches have been advocated, most of which can be successful if properly applied.
The decision-making depends on:
-
the cost of the restorative procedures
-
the risks of tooth fracture
-
the aesthetic requirements of the patient
-
the success of the root canal treatment or retreatment.
The impact of the cost of the restorative procedures will not be considered in this book. Affordability must always be viewed in the context of the best interests of the patient.
The amount of sound tooth structure remaining after root canal treatment and the amount of tooth structure which is lost during crown preparation are important factors in planning the design of post-endodontic restorations. Existing literature suggests a close relationship between the amount of remaining tooth structure and the fracture resistance of the restored endodontically treated tooth.
It is therefore of paramount importance to preserve as much sound tooth structure as possible. The use of minimal preparation techniques and adhesively retained restorations should be considered whenever possible.
Anterior teeth are less susceptible to fracture and more demanding aesthetically than posterior teeth. As a consequence, the restoration of anterior and posterior teeth will be treated separately.
Anterior Teeth
The life expectancy of a root canal treated anterior tooth is not always increased by preparation and coverage with a crown. Full coronal coverage is indicated:
-
if the amount of remaining tooth structure is not sufficient for restoration by direct methods (Fig 3-1a–h)
-
when aesthetics are critical
-
when anterior teeth are to be used as abutments of bridges.

Fig 3-1 (a) and (b) Crown fracture of the upper left central incisor. (c) Root canal treatment and crown build-up. (d) Crown preparation. (e) Ceramic try-in. (f–h) Final result.
Restorative Options for Anterior Teeth
Composite filling
Where proximal and incisal tissue loss represents less than one third of the coronal tooth structure, direct composite restoration is usually the method of choice. Bleaching techniques can be used to solve mild discoloration problems.
Ceramic or composite veneer
Ceramic or composite veneers are an option for restoring appearance and function when the extent of tissue loss is less than one third of the coronal structure, the palatal aspect of the tooth is preserved and it is impossible to obtain a good aesthetic result by direct means. Usually, veneers cover the entire labial surface and may extend over the incisal edge and through the proximal contacts. Veneers cannot realistically be extended to incorporate the endodontic access cavity. Partial ceramic or composite crowns are rarely constructed for root-filled anterior teeth as they may be compromised by the technical challenges of incorporating the endodontic access.
Metal-ceramic crowns
Metal-ceramic crowns remain the most commonly prescribed indirect restorations for root canal treated anterior teeth. In order to secure adequate aesthetics a buccal surface reduction of approximately 1.8–2.0 mm must be achieved (Figs 3-2 and 3-3). This may seriously compromise the strength of any remaining tooth tissue, and caution should be exercised before prescribing restorations, which contrary to supporting the residual tooth tissue may promote its loss.
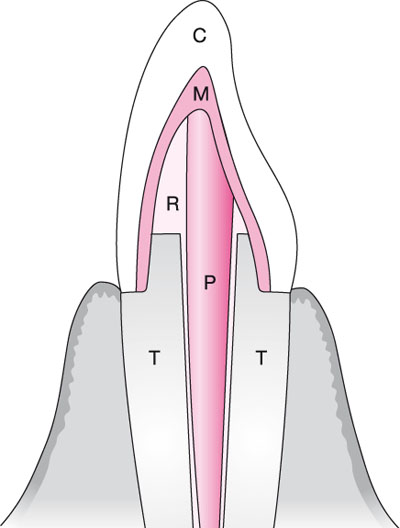
Fig 3-2 Schematic drawing of a tooth restored using a post and a metal-ceramic crown. C, ceramic; M, metal; R, composite core; P, post; T, residual tooth structure.

Fig 3-3 Thickness required for different crown materials (mm).
Captek Auro Galva Crown, Sintercast
These techniques offer two advantages:
-
The buccal tooth reduction required (0.8–1 mm) is less than that needed for a metal-ceramic crown, with potential benefits in terms of strength and tooth preservation.
-
The colour of the underlying gold allows a better aesthetic result, in particular, in the cervical area. (Fig 3-4).
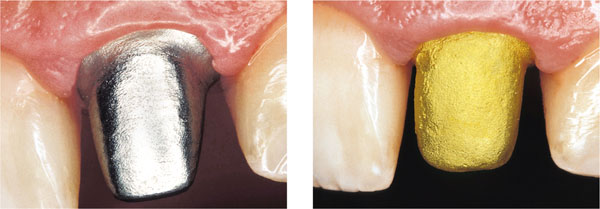
Fig 3-4 The aesthetics of soft tissues is influenced by the colour of the metal used for the core.
All-ceramic crowns
Advantages of all-ceramic crowns include:
-
More conservative buccal tooth reduction than required for metal-ceramic crowns (Fig 3-5).
-
Improved aesthetics, especially in areas close to the soft tissues (Fig 3-1e), resulting from the absence of a metal substructure.
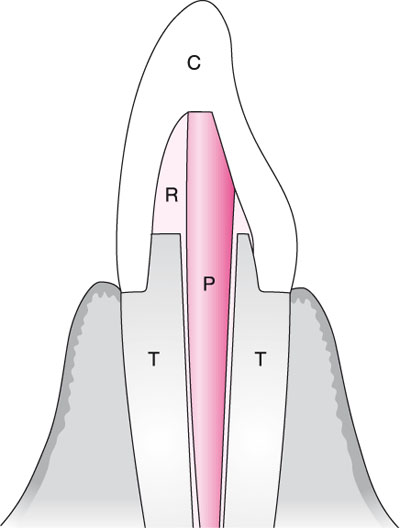
Fig 3-5 Schematic drawing of tooth restored using a post and an all-ceramic restoration. C, ceramic; R, composite core; P, post; T, residual tooth structure.
Endodontically treated teeth are often discromic; therefore, opaque ceramic cores are indicated (Fig 3-6a–f).

Fig 3-6 (a–f) Improving aesthetics. The crowns on the maxillary central incisors are unsatisfactory because they are too translucent (a). The two central incisors were re-prepared (b,c). New crowns were constructed using a more opaque material (d–f).
All-ceramic crowns are more fragile than metal-ceramic crowns. As abutments for bridges, they are only indicated for three-unit bridges in cases of high aesthetic need. A zirconium construction is indicated in such cases (Fig 3-7).

Fig 3-7 Bridge made using all-ceramic crowns reinforced with zirconia.
Gold-resin crowns
Gold-resin crowns have been abandoned due to inadequate aesthetics and the high cost of gold.
Resin crowns
Some authors have suggested the use of all-resin crowns to:
-
minimise the removal of sound tooth structure (typical reduction 0.8–1 mm)
-
allow an optimal aesthetic outcome, in particular, where margins are placed subgingivally
-
allow an adhesive cementation.
Unfortunately, resin crowns are just as expensive as metal-ceramic and all-ceramic crowns, but nowhere near as durable.
Posterior Teeth
Endodontically treated posterior teeth are subject to cuspal wedging, high compressive loads and shearing forces, and may, as a consequence, be at high risk of fracture. Cuspal coverage is indicated therefore, especially when one or more marginal ridges are lost. Most clinical studies have concluded that the survival of root canal treated posterior teeth is significantly higher when complete cuspal coverage is provided. Root canal treated teeth crowned as single units survive longer than bridge abutments.
Clinical Choices for Posterior Teeth
Amalgam restoration
-
A conventional amalgam, including wide interproximal extension and no cusp coverage is contraindicated, given the acknowledged high risk of cuspal or root fractu/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


