The Patient Record
Learning Outcomes
On completion of this chapter, the student will be able to achieve the following objectives:
• Pronounce, define, and spell the Key Terms.
• Identify the importance of a patient record.
Performance Outcomes
On completion of this chapter, the student will be able to meet competency standards in the following skills:
• Oversee the completion of a new patient registration form.
• Obtain a completed medical-dental health history form for a new patient.
• Record a completed dental treatment.
• Demonstrate how to make corrections on a patient’s record.
Electronic Resources
 Additional information related to content in Chapter 26 can be found on the companion Evolve Web site.
Additional information related to content in Chapter 26 can be found on the companion Evolve Web site.
Key Terms
Alert To bring attention to a specific medical or clinical condition.
Assessment The process of collecting data and then evaluating or drawing conclusions from the findings.
Chronic Persisting over a long time.
Chronologic Arranged according to the time of occurrence; earliest to most recent.
Forensic (fuh-REN-zik) Pertaining to the identity of an individual on the basis of scientific methods.
Litigation (li-ti-GAY-shun) Act of initiating legal proceedings, as in a lawsuit.
Quality assurance Program in place for monitoring and evaluating a project, service, or facility to ensure that standards of quality are being met.
Registration Act of completing forms by providing personal information.
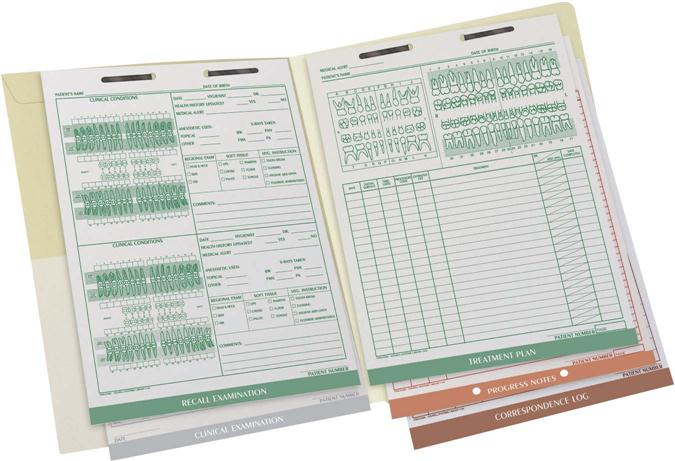
The patient record is the most important document maintained for each patient in a dental practice (Fig. 26-1). Whether you are communicating with a patient by phone or in person, the patient record must be available to refer to. A patient’s record is organized in a specific order to allow the dental team to move from the patient’s personal information, to the diagnostic findings, and then finally to the documentation of treatment.
Information-gathering forms are to be completed by the patient with the assistance of the business assistant before any treatment is provided (Fig. 26-2). These include the following:
• Patient registration form (personal patient information)
• Medical-dental health history form (patient’s overall health and dental status)

The patient will be escorted to the clinical setting, where the dental assistant or the dental hygienist along with the dentist will complete the following Diagnostic information–gathering forms:
• Physical examination form (posture and gait, vital signs, cognition, and communication skills)
• Clinical examination form (extraoral examination, intraoral examination, periodontal examination)
Once the diagnostic information–gathering process has been completed, the dentist will formulate an assessment from the findings of oral health status. An assessment is the process of collecting data and then evaluating or drawing conclusions from the findings. During this stage, the dentist will complete the following:
• Review all significant findings
• Present a diagnosis to the patient
• Develop and document a treatment plan with input from the patient
• Schedule a series of appointments by which to complete treatment in a timely manner
• Follow through with maintenance stages of the patient care process.

Patient Compliance
A patient record contains confidential information related to a patient’s personal background. It is important for the dental team to follow a high standard when documenting and handling this information. Besides its use in the clinical care of a patient, the patient record can have legal significance, of which the dentist and staff must be aware.
Permanent Record
The patient record is a permanent document of the dentist. This permanent document, also considered a legal document, can be used as (1) evidence in a legal settlement or lawsuit; (2) a reference tool in a forensic case for identification of an individual with the use of a patient’s radiographs or study casts; or (3) a reference for appropriate third parties, such as dental insurance companies and government-aided programs.
Privacy
HIPAA requires that all dental practices today have a written privacy policy. This written policy must inform the patient that the office will not use or disclose protected health information (PHI) for any purpose other than treatment, diagnosis, and billing. The privacy policy is prepared in a written format and must be provided to every patient; all patients must review and sign an acknowledgment that they have received notice of privacy practices (Fig. 26-3). This signed acknowledgment is kept in the patient’s record for a minimum of 6 years. See Chapter 4 for additional legal information regarding HIPAA.
Quality Assurance
The dentist will use the patient record as the primary source of information in determining the overall quality of care that a patient receives. Quality is the key word to remember when a patient is receiving dental care.
Does the patient believe that the best and most timely treatment is being provided? This question can be extremely important if the clinical setting is a larger practice with multiple practitioners, or a community dental clinic or teaching institution, where patients may be seen by different dentists. Each dental setting must promote an efficient and effective quality assurance program. Following are examples of ways to provide quality assurance in your dental office:
• Routine forms are completed by each patient and verified with his or her signature and date.
• Timely “recall” of patients is followed to address their dental needs.
• A completed patient record is kept for each “active” patient in the dental practice.
• Documentation includes information on when radiographs were taken.
• Current and up-to-date emergency standards are adhered to by the dental team.
Risk Management
As was noted earlier, the patient record provides documentation regarding a patient’s clinical findings, diagnosis, treatment plan, and response to treatment. For the dentist to avoid litigation such as a malpractice suit in the process or outcome of treating a patient, patient records must be kept organized and complete. For additional information on risk management, see Chapter 5.
Research
A complete and chronologic order of a patient record, or of a specific dental condition/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


